





Abstract
A 64-year-old male presented with a 2-month history of sudden onset dysphonia. Endoscopic evaluation of the larynx revealed a complete right vocal cord palsy. Computed tomography of the neck revealed a mass medial to the right thyroid associated with the cricoid cartilage. Histologic examination confirmed high-grade chondrosarcoma. The patient underwent right-sided hemicricoidectomy with tracheal flap reconstruction, right thyroid lobectomy and partial oesophagectomy with primary anastomosis followed by adjuvant radiation therapy. He is currently being followed as an outpatient with no evidence of disease. High-grade chondrosarcoma of the larynx is an exceedingly rare tumour, associated with a poor prognosis. Current best evidence suggests primary surgical resection with negative margins. There is a lack of evidence to guide post-operative management of high-grade chondrosarcoma. They have a poor prognosis following surgical resection and a 10-year survival rate of 29%.
INTRODUCTION
Chondrosarcoma of the larynx is a rare tumour and accounts for 1% of all laryngeal cancers. While most chondrosarcomas are low-to-intermediate-grade, 5–10% are high-grade and are associated with a poor prognosis. We describe a case of high-grade chondrosarcoma of the larynx presenting with dysphonia in a 64-year-old man.
CASE REPORT
A 64-year-old man presented with a 2-month history of sudden onset dysphonia, but did not describe a history of dysphagia or weight loss. The patient had history of ischaemic heart disease, chronic obstructive pulmonary disease and was an ex-smoker of 5 years with a 120 pack-year smoking history.
Physical examination revealed no evidence of disease within the oral cavity or cervical lymphadenopathy. Nasoendoscopic evaluation of the larynx revealed a complete right vocal cord palsy but no obstructing airway lesion was identified. Contrast enhanced computed tomography (CT) of the neck revealed a bi-lobed cystic mass (2.0 × 1.3 cm2) medial to the inferior lobe of the right thyroid associated with the cricoid cartilage causing displacement of the oesophagus (Fig. 1).
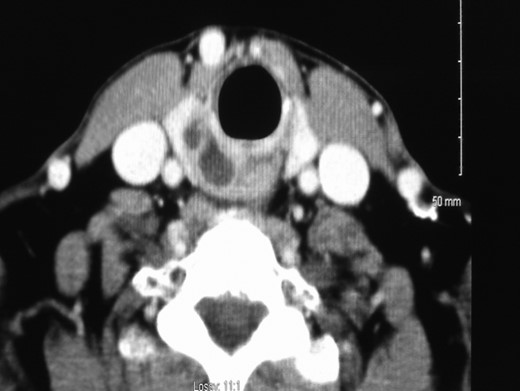
Contrast enhanced computed tomography of the neck showing a bi-lobed cystic mass (2.0 × 1.3 cm2) medial to the inferior right lobe of right thyroid associated with the cricoid cartilage causing displacement of the oesophagus.
Ultrasound guided fine needle aspirate (FNA) was performed. Histology confirmed high-grade chondrosarcoma.
The patient was diagnosed with high-grade chondrosarcoma of the larynx. He underwent surgical resection of tumour including right side of cricoid cartilage, right lobe of thyroid, partial oesophagectomy with primary anastomosis and reconstruction with a tracheal rotation flap.
Histologic evaluation revealed high-grade chondrosarcoma originating from the cricoid cartilage, with local invasion of the surrounding right lobe of thyroid gland (Fig. 2). Tumour was present at one margin in the external thyroid muscle. There was no tumour present in the oesophagus.
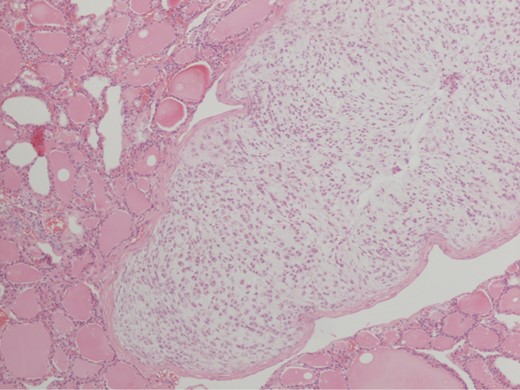
Pathological specimen showing high-grade chondrosarcoma invading into surrounding right lobe of thyroid gland using hematoxylin and eosin stain under ×10 magnification.
Post-operative recovery was uneventful. He was discharged and is currently well with no evidence of disease. Due to the aggressive nature of the tumour and a histological R1 resection, the patient received adjuvant radiation therapy to the neck. He is currently alive with no evidence of recurrence.
DISCUSSION
Chondrosarcoma are mesenchymal tumours originating in bone or cartilage. Laryngeal chondrosarcoma accounts for 1% of laryngeal cancers with 80% originating from cricoid cartilage [1]. The most common presentation of laryngeal chondrosarcoma is hoarseness. Most chondrosarcomas (90–95%) are low grade and do not behave in an aggressive fashion [2]. However, high-grade chondrosarcoma may rarely occur and are associated with a higher metastatic potential, 70%, compared to the low-grade tumours [3]. They have a poorer prognosis following surgical resection and a 10-year survival rate of 29% [3, 4].
Chondrosarcoma are classified under the World Health Organization (WHO) classification system for Atypical Cartilaginous Tumours. The grading system is on a scale of 1–3 and looks at mitotic activity, nuclear size and degree of cellularity [5].
Sarcomas of the head and neck usually present with local disease. Local invasion occurs in 10–15% of all head and neck sarcomas, mostly occurring with high-grade lesions. Distant metastases are uncommon, especially in the absence of local invasion.
Management of laryngeal sarcomas involves excision of the primary tumour with clear resection margins. Due to the slow-growing behaviour of most chondrosarcoma, conventional radiotherapy is relatively ineffective [6]. However, it may be beneficial as adjuvant therapy following margin positive resection (R1) of disease or when used with palliative intent. One study showed adjuvant radiation therapy provided local control in 94% of R1 resections, median follow-up 75 months. However, this study cohort comprised mostly of grade 1 and 2 tumours with only 14% being grade 3 [7].
There is some evidence supporting the use of alternative radiation therapy modalities. Proton beam irradiation allows for higher does of radiation to be given to directly to the target tissue with considerably less ‘scatter’ radiation to the surrounding tissues, when compared to conventional radiation therapy. Proton beam irradiation has been used to treat chondrosarcomas and chordomas of the skull base, where residual tumour remains following surgical resection [8]. Proton beam therapy provided local control rates of 92 and 76% for chondrosarcomas and chordomas, respectively. Tumours involving the brainstem had a local control rate of 53% due to necessary dose reduction due to brainstem tolerance constraints. Unfortunately, proton beam therapy is not readily available in the UK and Ireland.
There is little data on the effectiveness of chemotherapy in treatment of high-grade chondrosarcoma. No randomized controlled trials have been conducted. Chondrosarcoma are rare tumours, especially those of grade 2 or 3, so the few prospective studies are small. Low-grade chondorsarcoma are considered relatively chemo-resistant due to their slow growing nature, poor vascularity of the tumour and the expression of multidrug-resistance-1 gene [9]. Retrospective studies have suggested that chemotherapy may be of benefit in patients with unresectable disease. One study found that systemic treatment significantly improved survival, when compared with no treatment [10]. However, the overall survival rate for all patients was poor at roughly 50% per annum.
Specific data on chondrosarcoma of the larynx is limited by the size of the studies. The largest study by Thompson and Gannon had only 111 patients [1]. Of these 111 patients, only 6 were high-grade (grade 3).
In summary, high-grade chondrosarcoma of the larynx is an exceedingly rare tumour associated with a poor prognosis. Current best evidence suggests primary surgical resection with negative margins. Chemotherapy may provide some benefit where surgery is not an option. There is a lack of clinical evidence on the best post-operative management of high-grade laryngeal chondrosarcoma
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.

{kind=link}
{kind=link}