





Abstract
Right or subtotal colectomy either open or laparoscopic may be a challenging operation owing to technical difficulties. One of these, is to identify a safe and adequate dissection plane, ligating and dissecting lymph nodes around middle colic vessels. The purpose of this study was to depict a rare anatomic variation of middle colic vein (MCV) draining to splenic vein. We report the case of a 55-year-old male patient, who was subjected to a right hemicolectomy for an adenocarcinoma in the ascending colon. During dissecting the transverse mesocolon from the greater omentum, for complete mesocolic excision (CME), we encountered that the MCV drained in the splenic vein. With respect of this rare anatomic variability, CME was completed without hemorrhage. Our aim is to depict that deep knowledge of MCV anatomy and its variations is of paramount importance to achieve CME and to avoid dangerous or massive bleeding.
INTRODUCTION
Surgery remains the fundamental radical treatment of colon cancer. Long-term prognosis can be improved by improving the surgical treatment without increasing the risk of perioperative mortality. Complete mesocolic excision (CME), is the surgical strategy of a more extensive lymph node (LN) dissection when a right hemicolectomy is performed. There are studies that have shown that CME is associated with better oncological outcome and without increased risk of perioperative mortality [1].
To achieve an optimal oncologic resection, wide excision of the mesocolon close to the pancreas is required. Unexpected bleeding around the pancreas is sometimes difficult to control. As a result, surgeons should know precisely the embryology and anatomy of the mesenteric circulation and its variations.
Variations in the mesenteric circulation, are a result of varying degrees of persistence of certain portions of the dual blood supply in the primitive fetal blood supply. During subsequent differentiation, much of this dual vascular supply regresses [2].
The anatomic course of middle colic vein (MCV) follows that of the middle colic artery. It normally drains the transverse colon into the superior mesenteric vein (SMV) and in close proximity to the inferior border of the pancreas. MCV may be encountered during the medial portion of the dissection.
Injury to the MCV may lead to unnecessary blood loss and increased operative time during right hemicolectomy. If recognized, the MCV may be ligated with safety if it is injured or torn because there is an adequate network of collateral venous drainage for the large intestine [3].
During the course of dissection, MCV and SMV should be identified and spared from injury. Ideally, the course of these vessels must be known preoperatively, as proposed by Ogino et al. [4].
CASE REPORT
We report the case of a 55-year-old male patient who presented in our Department with symptoms of weight loss and anemia. Colonoscopy revealed a 3 cm tumor in the ascending colon. Histology revealed an adenocarcinoma of poor differentiation. Staging with abdominal computer tomography was negative for metastasis. Tumor markers where within normal range.
The patient was subjected to open right hemicolectomy. During the operation, the right colon was mobilized and resected with a GIA stapler and a side to side ileotransverse anastomosis was performed in two layers.
We report, that during dissecting the transverse mesocolon from the greater omentum, and while performing LN dissection around the middle colic vessels, in accordance with the principles of CME, we encountered the following anatomical variability. In this patient, the MCV drained in the splenic vein (Fig. 1). With respect of this rare anatomic variability, CME was completed without hemorrhage (Figs 1 and 2).
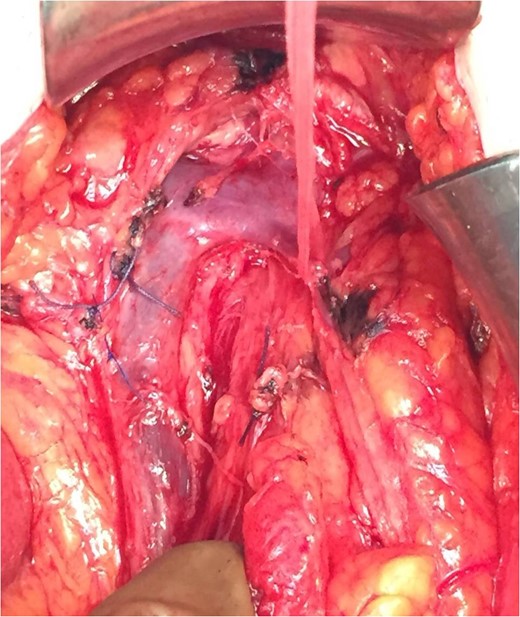
It is depicted the principal finding of our case, the anatomic variation of the middle colic vein draining to splenic vein.

The venous anatomy of the right colon in our case.
The patient was discharged 8 days after surgery and had a good post-operative course.
The final diagnosis was confirmed as adenocarcinoma, T3, N2a, M0, Stage IIIB. The resection was on clear margins. Due to the presence of LN metastasis, adjuvant chemotherapy was recommended.
DISCUSSION
Bleeding may be a major complication during right hemicolectomy and when mobilizing the right colon and dissecting the SMV at the inferior border of the pancreas. This bleeding is caused by small vessels near the head of pancreas or when expecting an anatomic variability [5].
The reason for this is attributed to the fact that this anatomic area is covered by the omentum and the transverse mesocolon.
Excessive or inadvertent traction may be the cause of tearing the fragile veins. These usually need to be sutured, and on rare occasions the tearing may be lethal [5].
In addition, CME, based on the same principle as total mesorectal excision, exhibits 15% better 5-year overall survival compared with mesocolic defect surgery [4, 6]. To perform right hemicolectomy in CME, adequate mobilization of the right colon, complete LN dissection along the surgical trunk, and complete resection of the mesocolon are important [4, 7].
The aim of this case report is to investigate the anatomic basis of this problem and to shed light on venous variations of the right colon. Our emphasis was to MCV and to investigate the usefulness of this anatomic knowledge during CME for right colon cancer.
In a study of Ogino et al. [4] the main MCV flowed into the SMV in 68% of patients, gastrocolic trunk (GCT) in 20%, jejunal vein in 6%, inferior mesenteric vein in 5%, and the splenic vein in 1% of patients as in our case [4]. The GCT was present in 88% of patients. The gastrocolic trunk of Henle (GTH) is the confluence of the superior right colic vein (SRCV) and the right gastroepiploic vein draining into the SMV [5].
In other anatomic studies in cadavers, Yamaguchi et al. [8], have reported that in 2 cadavers out of 58 (2/58), there was anomalous drainage of the main MCV to the splenic vein and to the inferior mesenteric vein [8].
To conclude, venous variation of the right colon is high. Preoperative evaluation is informative and helpful for surgeons performing open or laparoscopic CME for right colon cancer, when dissecting near the inferior border of the pancreas. Ideally, information obtained from this study with anatomic variability should be applicable preoperatively or at least intraoperatively for individual cases. To avoid lethal bleeding or other major complications by violating the venous anatomy of the right colon during CME, optimizes oncologic safety.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no conflict of interest.
FUNDING
All authors declare that are no funding requirements.

{kind=link}
{kind=link}