





Abstract
Complications related to cholecystectomy occur in <3% of patients. Endoclip migration after laparoscopic cholecystectomy with hepatolithiasis is an extremely rare complication. We report a case of hepatolithiasis secondary to endoclip migration after laparoscopic cholecystectomy treated successfully via right hepatectomy. A 35-year-old female presented with upper abdominal pain, fever and vomiting 9 years after laparoscopic cholecystectomy for chronic calculus cholecystitis. Laboratory investigation revealed gamma-glutamyl transpeptidase of 550 U/L and alkaline phosphatase of 350 U/L. Magnetic resonance cholangiopancreatography revealed a dilated intrahepatic bile duct in segment 6 filled with stones. After preoperative evaluation, a right hepatectomy was performed using the intermittent Pringle maneuver. The postoperative recovery was uneventful and the patient was well after 4 months of follow-up. Although rare, endoclip migration should be considered in patients presenting with intrahepatic lithiasis even many years after laparoscopic cholecystectomy. Liver resection may be necessary in cases of failure of endoscopic extraction.
INTRODUCTION
Laparoscopic cholecystectomy is the gold standard of treatment for symptomatic gallstone disease. Complications related to cholecystectomy occur in <3% of patients [1]. Hepatolithiasis is the presence of gallstones in the bile duct proximal to the confluence of the hepatic ducts. The exact incidence is unknown. Many conditions have been associated with hepatolithiasis, including genetic, dietary and environmental factors. Endoclip migration after laparoscopic cholecystectomy is a rare complication and can occur years after the procedure. Surgical endoclip into the bile duct can promote biliary occlusion and serve as a nidus for stone formation. In most reported cases, the complication is choledocholithiasis and subsequent biliary obstruction with acute or recurrent cholangitis. Hepatolithiasis due to endoclip migration into the bile duct is an extremely rare complication, and to the best of our knowledge, this is the first case of a migrated endoclip resulting in occlusion of the segment 6 duct after laparoscopic cholecystectomy [2, 3]. This study reports a case of hepatolithiasis in the segment 6 duct secondary to endoclip migration after laparoscopic cholecystectomy. The patient was successfully treated with right hepatectomy.
CASE REPORT
A 35-year-old female presented with upper abdominal pain, fever, nausea and vomiting for 3 days. She had undergone uncomplicated laparoscopic cholecystectomy 9 years earlier for chronic calculus cholecystitis and endoclips had been used to ligate the cystic duct and cystic artery.
Physical examination revealed right hypochondrial tenderness but was otherwise unremarkable. Laboratory investigation revealed normal bilirubin, aspartate aminotransferase, and alanine aminotransferase, and gamma-glutamyl transpeptidase of 550 U/L (normal up to 50 U/L) and alkaline phosphatase of 350 U/L (normal up to 120 U/L). Abdominal ultrasound revealed a dilated intrahepatic duct with stones, but no extrahepatic stone was observed. Abdominal computed tomography showed stones within a dilated intrahepatic bile duct of segment 6 and a small radiopaque image with metallic density (Fig. 1). Magnetic resonance cholangiopancreatography (MRCP) revealed a dilated intrahepatic bile duct of segment 6 filled with stones. A single filling defect in the distal common bile duct was also observed (Fig. 2). The case was discussed at a hepatobiliary meeting. Due to the difficult position of the stones (segment 6), endoscopic retrograde cholangiopancreatography was not possible and liver resection was indicated. The patient underwent surgery after preoperative evaluation.

Abdominal computed tomography with stones.

MRCP dilated intrahepatic bile duct with stones.
A modified Makuuchi incision was used, and during the dissection at the level of lowering the hilar plate, two endoclips were identified (Fig. 3a and b). Right hepatectomy was performed. The liver was mobilized and the right pedicle was dissected, ligated and divided. Transection of the liver parenchyma was performed using bipolar coagulation irrigated with saline solution with the intermittent Pringle maneuver. Right hepatectomy was performed (Fig. 4). Two silicone drains were placed, and the abdomen was closed. The operating time was 188 min, the blood loss was 450 mL, and no blood transfusion was necessary. The postoperative recovery was uneventful, and the patient was discharged 6 days after the procedure. The patient was well after 4 months of follow-up.
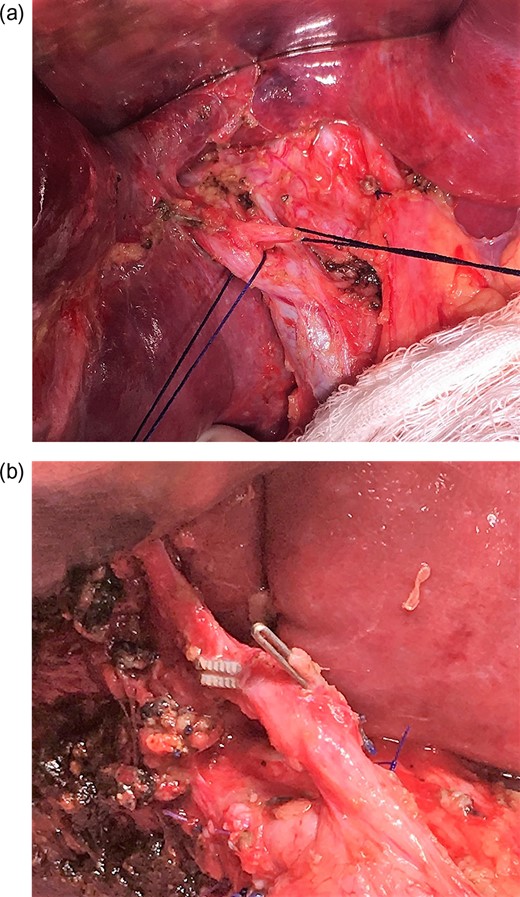
(a and b) Two endoclips identified.
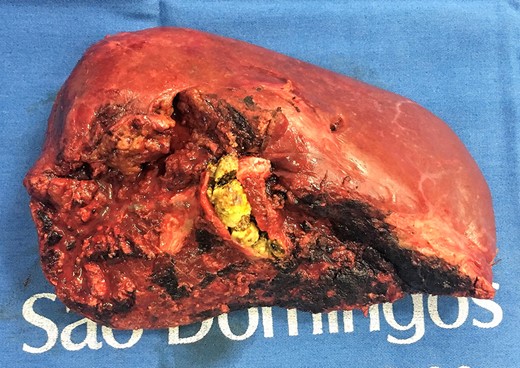
Right hepatectomy (with stones).
DISCUSSION
Laparoscopic cholecystectomy is the gold standard treatment for symptomatic gallstone disease. Since its introduction, surgical endoclips have been routinely used to control the cystic duct and the cystic artery and their use is considered effective and safe. Migration of endoclips after cholecystectomy is a rare and well-documented complication [1, 2, 4].
The incidence of this complication is unknown, and we believe that endoclip migration is more common when laparoscopic cholecystectomy is performed for acute cholecystitis. A variety of endoclip-related complications has been described, such as obstructive jaundice, cholangitis and acute pancreatitis. The case presented herein is unique because stone formation occurred in the segment 6 duct due to endoclip migration [2, 3, 5]. To the best of our knowledge, this is the first case of a migrated endoclip resulting in occlusion of the segment 6 duct after laparoscopic cholecystectomy.
The mechanism of endoclip migration is not clearly understood but may be a complex process involving inflammation around the cystic duct and ineffective clip placement leading to incomplete closure. The protruding or compression of a migrated endoclip in the common bile duct or hepatic duct can serve as a nidus and promote stone formation [3, 5, 6]. In the present case, the endoclips had probably migrated, leading to compression of the segment 6 duct above the cystic duct, followed by stone formation.
Short cystic duct, clip placement close to the common or segmental bile duct, manipulations after clipping (irrigation and aspiration), and local ischemia are also risk factors for endoclip migration. Inadvertent placement of endoclips inside the common bile duct or hepatic duct during cholecystectomy and the placement of many clips on the cystic duct stump have also been suggested. Rejection response to surgical endoclips may contribute to the migration process [2, 5, 7]. In our study, cholecystectomy was performed for chronic cholecystitis and resulted in ineffective closure of the cystic duct.
The time interval between the initial cholecystectomy and the development of complications due to endoclip migration varies from some days to 20 years. The symptoms may include abdominal pain, nausea, vomiting, anorexia, pruritus, jaundice and fever due to ascending cholangitis [3, 4, 7].
Computed tomography and MRCP are useful for the diagnosis of complications following laparoscopic cholecystectomy. MRCP provides a clear evaluation of the biliary tree with a high sensitivity and specificity [4, 7, 8].
Endoscopic sphincterotomy (ES) and stone or clip removal should be the procedure of choice and the success rate is close to 80%. Surgery is reserved as rescue procedure mainly in the presence of intrahepatic stones or biliary stricture with large stones when ES was not effective. In this case, due to the difficult position of the stones, ES was not indicated, and liver resection was the procedure of choice [9, 10].
To reduce the incidence of endoclip migration, the following technical approaches during the surgery should be emphasized: confirming the correct anatomy of Calot’s triangle during dissection, accurate endoclip placement, reducing the number of endoclips, placing endoclips away from the common bile duct or hepatic duct and avoiding unnecessary procedures. Further, absorbable endoclips or absorbable sutures are safe and effective instruments [3, 4, 6, 7, 8].
CONCLUSIONS
Although rare, endoclip migration should be considered in the differential diagnosis of patients presenting with intrahepatic lithiasis even many years after laparoscopic cholecystectomy. ES is currently the treatment of choice, but liver resection may be necessary in cases of failed endoscopic extraction.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}