





Abstract
Cholecystitis is a common gallbladder pathology characterized by abdominal pain, positive Murphy sign and elevated white blood count. Abdominal ultrasound usually gives a definite diagnosis. Duplication of the gallbladder is a rare congenital anomaly that can either be asymptomatic or and can present with symptoms associated with cholelithiasis, cholecystitis, cholangitis or pancreatitis. Clinically indistinguishable from regular gallbladder pathologies. The management of duplicated gallbladder is similar to that of other gallbladder diseases, if one or both gallbladders cause symptoms, cholecystectomy should be done for both gallbladders. We present a case of a 50-year-old female patient, she presented to the emergency room with abdominal pain and tenderness. Ultrasound detected a gallbladder duplication with cholecystitis in one of them and magnetic resonance cholangiopancreatography confirmed this diagnosis. Surgery was decided and the patient underwent full recovery. Y-shaped gallbladder duplication with cholecystitis due to cholelithiasis in one of them was the final diagnosis.
INTRODUCTION
Duplication of the gallbladder is a rare congenital anomaly [1]. They can appear from two origins, as split primordium or as an accessory gallbladder [2, 3]. They can be either asymptomatic, as there are no specific symptoms attributable to a gallbladder duplication [4], or and can present with symptoms associated with cholelithiasis, cholecystitis, cholangitis or pancreatitis [3, 5]. Surgery is the treatment of choice for symptomatic cases [3]. We present a case of a 50-year-old female patient with a gallbladder duplication and cholecystitis in one of them. Surgery was decided and the patient underwent full recovery.
CASE REPORT
Patient is an otherwise healthy 50-year-old female adult, without any past medical history. She presented to the emergency room with fever and epigastric pain, having experienced 3 months of an intermittent pain in the right upper quadrant that was related to fatty food intake. Abdominal examination showed upper abdominal tenderness and a positive Murphy sign.
Laboratory data found elevated white blood cell count and a positive C-reactive protein. Bilirubin, liver function tests and amylase were normal. Due to pain, an abdominal ultrasound was requested that revealed two gallbladders. Two piriform images, with anechoic content, were detected. The left one had gallstones and right one had biliary sludge, also the right gallbladder had a thickened echogenic 4.5 mm wall (Fig. 1A). A magnetic resonance cholangiopancreatography confirmed this diagnosis. It revealed a normal liver and a gallbladder duplication with inflammation signs in one of them (Fig. 1B), they both had independent cysts ducts that joined in a common cystic duct before entering a normal diameter common bile duct (Fig. 1C).

(A) Abdominal ultrasound revealing two gallbladders. (B) A magnetic resonance cholangiopancreatography revealing a normal liver and a gallbladder duplication with inflammation signs in one of them. (C) A magnetic resonance cholangiopancreatography revealing a gallbladder duplication with independent cysts ducts that joined in a common cystic duct before entering the common bile duct.
Gallbladder duplication with cholecystitis in one of them was suspected. Due to clinical, laboratory and images findings, surgery was decided.
At laparoscopy, multiple adhesions from omentum to the gallbladder fossa were seen and released, revealing the Calot’s triangle structures. After achieving critical view of safety, a gallbladder duplication was identified, the right gallbladder had purulent bile with thickening of its walls, the second gallbladder appeared normal. Both of them had independent cystic ducts, but only one cystic artery was detected (Fig. 2A and Supplementary Video). From there surgery was straightforward, clips were applied to the common cystic duct and cystic artery respectively and they were divided between the clips without any complications. After that, the gallbladders were dissected off the gallbladder fossa using electrocautery and retrieved in a latex bag via the umbilical port.
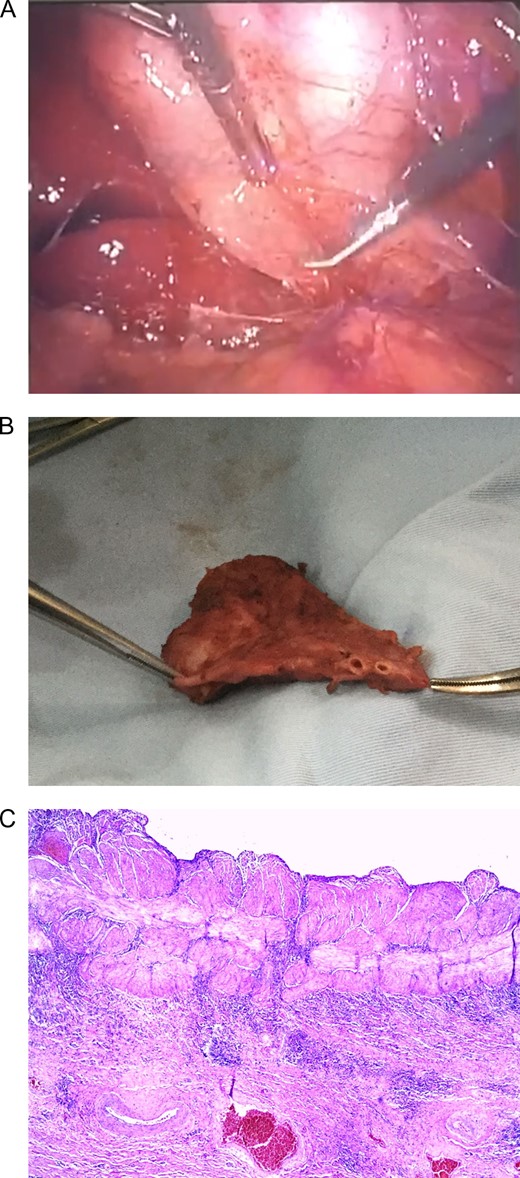
(A) Laparoscopic view of two gallbladders, each with its’s individual cyst duct and an oedematous wall in one of them. (B) Gallbladder duplication with two independent cystic ducts. (C) Thickened muscular layer and vascular congestion of gallbladder wall.
Pathology reported two permeable cystic ducts, and two separated gallbladders divided by thick inflammatory tissue. Multiple 0.5 cm gallstones were discovered in the left gallbladder and biliary sludge in the right one (Fig. 2B). Microscopically, chronic exacerbated cholecystitis was detected in the right gallbladder (Fig. 2C). A Y-shaped gallbladder duplication with cholecystitis due to cholelithiasis in one of them was the final diagnosis
The postoperative course of the patient was uneventful and she was discharged after full diet was tolerated.
Patient underwent full recovery, on follow-up controls patient is doing well.
DISCUSSION
Duplication of the gallbladder is a rare congenital anomaly, ever since Blasius et al. first decryption in 1675 [1] few cases have been reported [1, 2]. It is estimated that it occurs in every one of 3400 patients [2, 3]. This type of anomaly has not predominance over gender, age or ethnical predominance, and is commonly reported during surgical procedures and autopsies [5]. Gallbladder duplication can develop from two separated origins [2, 3].
As a split primordium, when there is only one cystic duct entering the common bile duct [1, 2], or as an accessory gallbladder; when two separate primordium arises on the biliary tree [3].
Multiple variants exist and a Y gallbladder is when two completely separate gallbladders, each with its own cystic duct form a common cystic duct before entering the common bile duct [2, 3]. This was discovered our case.
Because of associated anatomical variations of the cystic duct and hepatic artery, this congenital anomaly should always be in a surgeon’s mind [4]. Patients with gallbladder duplication can either be asymptomatic as there are no specific symptoms attributable to a gallbladder duplication [2, 5] or can present with symptoms associated with cholelithiasis, cholecystitis, cholangitis or pancreatitis [2, 3], as any gallbladder could be affected [5].
The ultrasonographic evaluation of the gallbladder, is by far the most useful diagnostic tool, it is highly sensitive in assessing gallstones, cholecystitis and detecting gallbladder anatomical abnormalities [6], and however in the setting of patient with duplicated gallbladder, ultrasound may not completely differentiate it from other pathologies; including Phrygian cap, choledochal cyst, folded gallbladder, among others [3, 4].
Further preoperative evaluation is usually recommended [3]. Magnetic resonance cholangiopancreatography, tomography, oral cholecystography, and HIDA scan can be useful for anatomical evaluation of the biliary tree [7]. This is particularly important in gallbladder duplication as the preoperative evaluation enables the surgeon to be aware of the type of anatomical variation and reduce the risks of complications from biliary and vascular injury including damage to the common bile duct or other important nearby structures [2, 3, 8]. However, only half of all patients have a correct preoperative diagnosis [8].
Our patient presented with abdominal pain and tenderness, after ultrasound evaluation a gallbladder duplication with cholecystitis was detected and a magnetic resonance confirmed this diagnosis.
The management of duplicated gallbladder is similar to that of other gallbladder diseases. Because there is no evidence of increased risk, surgery is not indicated for incidental discovered duplicated gallbladder, however, if one or both gallbladders cause symptoms, cholecystectomy should be done for both gallbladders [5, 7, 8]. Either by open or laparoscopic approaches [7, 8].
In our patient surgery was straightforward, after careful dissection, both gallbladders were completely resected and the patient successfully recovered.
A wide spectrum of diseases can affect the gallbladder, and duplication of the gallbladder, even if it’s rare, is one of them that which requires special attention due to the biliary ductal and arterial anatomy. Preoperative diagnosis and surgical awareness of the anatomic variations of the gallbladder and biliary system are critical for preventing lesions and reducing morbidity and mortality.
Surgeons always have to be aware of different forms of presentation of gallbladder pathologies even the ones that we are not used to seeing on daily basis.
SUPPLEMENTARY MATERIAL
Supplementary material is available at the Journal of Surgical Case Reports online.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}