





Abstract
Sodium polystyrene sulfonate, or Kayexalate, is an ion-exchange resin used to treat hyperkalemia. It is sometimes used with sorbitol, an osmotic laxative that prevents constipation. Small and large bowel necrosis and perforation due to Kayexalate were previously reported. However, no previous cases of gastric perforation were described. We present a case of gastric perforation in a 48-year-old patient, with chronic kidney disease (CKD), lung transplant under chronic corticosteroids, and two previous Nissen fundoplications. He presented with sudden epigastralgia, hematemesis and hemodynamic instability. Esophagogastroduodenoscopy was not able to localize the site of bleeding. Surgical exploration revealed perforation of the lesser curvature of the stomach. Antrectomy with a Billroth II reconstruction was performed. Pathological examination revealed no abnormalities except fibrinoleukocytic debris with Kayexalate crystals in the gastric wall. Kayexalate is believed to be a trigger for the gastric injury in a patient with tissues impaired by corticosteroids, CKD and immunosuppressors.
INTRODUCTION
Sodium polystyrene sulfonate (SPS), or Kayexalate, is an ion-exchange resin used to treat hyperkalemia. It is commonly administered to patients with chronic kidney disease (CKD), who present a chronic mild elevation of their potassium level [1, 2]. SPS is sometimes used with sorbitol, which acts as an osmotic laxative to relieve constipation and prevent fecal impaction [1–3].
Several cases of gastrointestinal necrosis, ulceration or perforation, mainly affecting the large and small bowel, were previously reported with Kayexalate [1, 4–6]. Only a few cases of gastric injury were described but no reports of gastric perforation due to SPS were published.
CASE PRESENTATION
A 48-year-old patient, hospitalized for a pulmonary multiresistant infection, presented with sudden upper gastrointestinal bleeding associated with hemodynamic instability. His past medical history includes high blood pressure, dyslipidemia, CKD, gastroesophageal reflux disease and a double lung transplant for emphysema 8 years ago. He was suffering from chronic rejection and treated with corticosteroids. His past surgeries include a laparoscopic Nissen fundoplication 5 years ago, which required an open reoperation for a symptomatic ‘slipped’ Nissen 3 months ago.
The patient experienced sudden severe epigastric pain and hematemesis. He responded well to initial fluid resuscitation, and underwent an urgent esophagogastroduodenoscopy that revealed a significant amount of blood in the upper digestive tract. The esophagus, duodenum and the Nissen site were free of bleeding lesions. The stomach was filled with ingested material and a large blood clot that prevented proper aspiration of its content. The source of bleeding could not be identified.
An X-ray of the abdomen showed free intraperitoneal air. A non-injected computed tomography of the abdomen and pelvis displayed important gastric distension with dense hematic content.
The patient became hemodynamically unstable and his abdomen significantly distended, suggesting a progressive compartment syndrome. He was taken to the operating room where surgical exploration reveals a 7 cm perforation of the lesser curvature of the stomach, coming into close proximity with the fundoplication site. This perforation was partially walled off by adhesions to the left lobe of the liver as well as adhesions to the diaphragm due to the redo Nissen. After proper evacuation of the blood clot and adequate hemostasis, an antrectomy with a Billroth II reconstruction were performed, without deconstruction of the previous fundoplication. The patient was discharged to the ward after a 7-day’ stay in the intensive care unit. On postoperative Day 12, he suffered an evisceration, which required a return to the operating room.
The resected gastric edges of the perforation site were sent for pathological examination, which revealed the presence of fibrinoleukocytic debris with rhomboid, birefringent crystals, suggestive of Kayexalate in the gastric wall (Fig. 1).
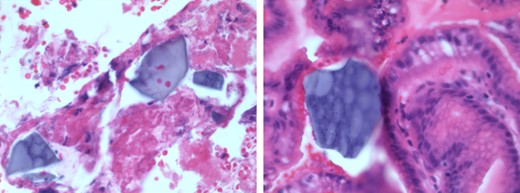
Foci of serositis and fibrinoleukocytic debris with rhomboid, birefringent crystals, suggestive of Kayexalate, in the gastric wall.
In absence of other acute objectified causes for the patient’s clinical presentation, Kayexalate is believed to be a significant contributing factor to the gastric injury in a patient with tissues weakened by several comorbidities.
DISCUSSION
We present the case of a 48-year-old patient with a gastric perforation that is possibly triggered by, among other things, Kayexalate ingestion.
Several cases of Kayexalate-associated gastrointestinal injuries have been previously reported. A systematic review of SPS-associated gastrointestinal events by Harel et al.[1] displays more than 50 cases of Kayexalate-induced adverse outcomes, presenting mainly as transmural colonic necrosis.
Three previous cases of gastric manifestations related to the use of SPS have been described. Gardiner [2] described patchy hemorrhagic erosions of the stomach, ileum and colon after administration of Kayexalate enemas and Kayexalate with sorbitol solutions via a nasogastric tube. In the same year, Roy-Chaudhury et al. [7] described a case of gastric and ileal serpiginous ulcers with the use of Kayexalate in sorbitol. Usta et al.[8] have recently reported a case of emphysematous gastritis and necrosis induced by oral ingestion of Kayexalate in sorbitol in a patient with acute kidney injury. To the best of our knowledge, no previous cases of gastric perforation due to SPS were reported.
Our patient seems to have sustained a significant gastric injury and a question is raised over the possible risk factors that have helped induce this injury. Harel et al.[1] present CKD, the postoperative state and transplantation as risk factors for SPS-associated gastrointestinal injury. In addition to CKD, our patient was on a chronic corticosteroid and immunosuppressive treatments. His tissues therefore are most probably weakened and their regenerative capacity decreased. Besides, with the recent gastric surgery, a question is raised over the perfect integrity of the gastric wall and its ability to cope with the additional stress SPS has inflicted upon it. Nonetheless, the evisceration the patient experienced sheds light on the tissues’ inability to heal properly, especially that their vascular supply is most probably also impaired. In fact, CKD is believed to induce an overactive renin–angiotensin–aldosterone system and consequently an increased renin level. This would in turn lead to vasoconstriction, a mechanism best known as non-occlusive ischemia in CKD patients [1, 2].
The role of sorbitol in gastrointestinal necrosis has long been controversial as it was thought to be the incriminated agent in reported cases of Kayexalate-associated injury. This non-absorbable sugar acts as an osmotic agent and is concomitantly used in SPS solutions to prevent constipation by drawing water into the bowel lumen. Recent papers have however suggested that SPS alone can be toxic as well, with sorbitol acting as a potentiating agent that promotes vasospasm and ultimately vascular injury [1–3, 9].
No histological abnormalities were objectified in the resected specimen and the previous Nissen site was intraoperatively perfectly intact. Nonetheless, assuming that Kayexalate alone is the sole trigger for the gastric perforation would be an oversimplification of a physiological process that involves most probably many incriminated factors in this case. However, its presence in the gastric wall raises a serious question over its safety in patients with risk factors for gastrointestinal adverse events.
In summary, the efficacy of SPS in treating hyperkalemia has been repeatedly challenged, and its effect even paralleled to simple laxatives and low-potassium diets [10]. Its pathogenic effect on the gastric wall, although very uncommon, still requires better characterization to be properly weighted against its benefits.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}