





Abstract
Appendiceal duplication is a rare congenital anomaly with an estimated incidence ranging from 0.004 to 0.009%. Preoperative diagnosis of a duplicated appendix is often difficult and is usually done intraoperatively. Histopathological examination of the surgical specimen is mandatory to confirm the presence of two appendices. In this case we report a female patient with acute inflammation in one of her two appendices. Surgeons should always bear in mind this rare anomaly to avoid serious ethical and legal consequences.
INTRODUCTION
The incidence of appendiceal duplication is reported to range from 0.004 to 0.009% [1, 2]. Until now more than 100 cases have been reported, of which <15 cases were complicated by acute appendicitis [3]. In this report we present a case of a duplicated appendix that was diagnosed in a female who presented with features of appendicitis requiring a laparotomy.
CASE REPORT
A 30-year-old female presented to the emergency department complaining of abdominal pain. The pain started 48 h ago diffusely in the umbilical region and subsequently migrated to the right iliac fossa. She had associated nausea, vomiting and loss of appetite. There was no alteration in bowel habits. The patient was otherwise healthy and has not undergone any previous abdominal or pelvic surgeries. On physical examination the patient was febrile (39°C) and tachycardic. Examination of the abdomen revealed localized tenderness as well as rebound tenderness at the McBurney point in the right iliac fossa. Laboratory findings showed severe leukocytosis (22 000/ul) with a left shift (neutrophils 88%), and increased C reactive protein (100 mg/dl). Urinalysis did not reveal any specific findings and urine pregnancy test was negative. Abdominal ultrasonography was performed and revealed an appendiceal shield, free fluid, and abscess formation in the right iliac fossa. A definite diagnosis of acute appendicitis was made based on Alvarado score of (10) and a decision was made to perform an open appendectomy via a Rocky Davis incision. Intraoperative findings showed a small quantity of free fluid in the abdomen and two appendices lying on either side of the ileocecal valve, one of them was swollen and erythematous (Fig. 1). The surgeon resected the two appendices. Histopathological examination confirmed the diagnosis of appendiceal duplication. The first specimen showed an inflamed appendix with lymphoid hyperplasia, thickened muscularis and prominent neutrophilic infiltration compatible with acute appendicitis (Fig. 2). The second specimen showed a normal appendix without serosal inflammation, or neutrophilic infiltrate in the muscularis propria (Fig. 3). The tip was present without any lesions. The patient had a full recovery without postoperative complications and was discharged on the third postoperative day.
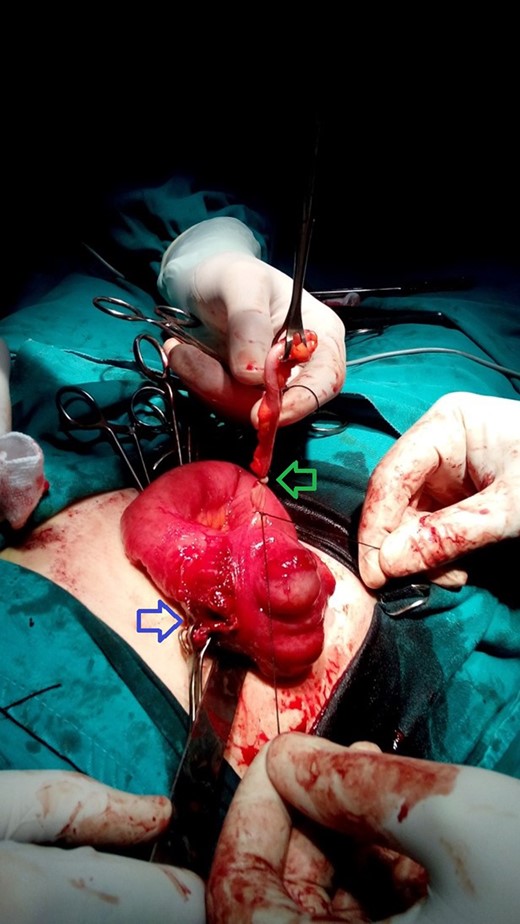
A photograph taken during surgery. Blue arrow indicates the site of inflamed appendix after resection. Green arrow indicates the second appendix.
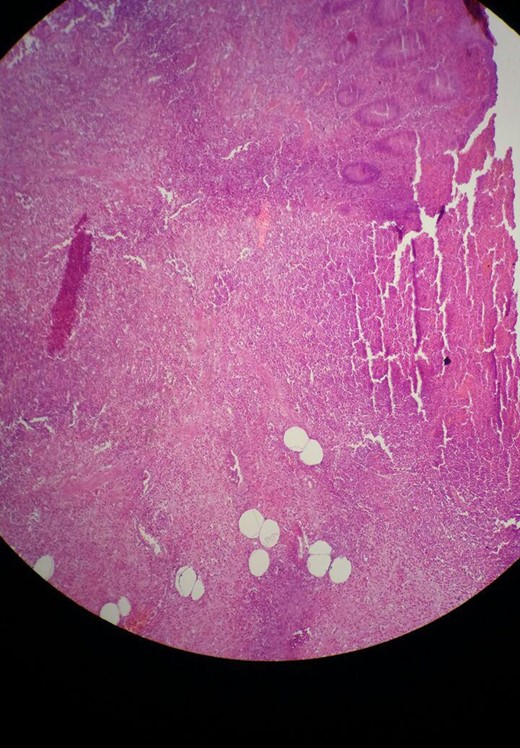
Microscopic view of the first specimen with acute appendicitis. Sections show focal ulceration of the mucosa and acute inflammatory infiltrate (mainly neutrophils) throughout the wall.
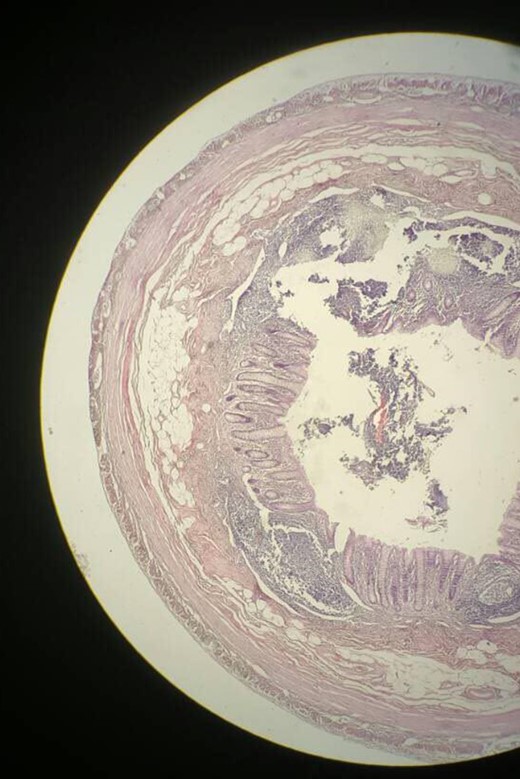
Microscopic view of the second specimen with a nearly normal appendix. Sections show a thin walled appendix lined by a colonic type glandular epithelium.
DISCUSSION
Despite the wide range of variations in the normal appendiceal position, the human vermiform appendix is rarely subject to the extremes of variation, absence and duplicity. Although the normal embryogenesis of the appendix is known, the exact cause of appendiceal duplication remains unclear [5]. Appendiceal duplication is a rare anomaly that was first described by Bartels in a fetal specimen in 1867 [4]. Picoli was the first to publish a case in 1892 [6], and more than a hundred cases with several variations have been reported until now [3]. The incidence of appendiceal duplication is estimated to range from 0.004 to 0.009% [1, 2]. Over time authors have presented classifications to categorize appendiceal duplication. The first classification was developed by Cave in 1936. Cave classified double appendices into types A, B and C [7]. This classification was modified by Waugh who further classified type B [8]. In 1963, Wallbridge added further modifications leading to the Cave Wallbridge classification which is now used widely [9]. This classification categorizes double cecal appendix into three types: A, B and C. Other extremely rare variations that do not fit into the above mentioned classification include the horseshoe appendix and the triple appendix. The modified Cave–Wallbridge classification and the frequency of each type of appendiceal duplication are shown in (Table 1) [4, 7–9].
| CW Type | Features | Frequency, n (%*) |
|---|---|---|
| CW Type A | Two appendices with a common origin from a single cecum | 22 (18) |
| CW Type B | Two appendices with different origins from a single cecum | 73 (59) |
| Type B1 | Two appendices placed symmetrically on either side of the ileocecal valve | 8 (6) |
| Type B2 | One appendix is in its usual position, second appendix arises alongside the tinea coli | 46 (37) |
| Type B unclassified | 19 (15) | |
| CW Type C | Two cecea each with a cecal appendix | 10 (8) |
| Horseshoe | One appendix has two openings into a common cecum | 6 (5) |
| Triple | One appendix arises from the cecum, two additional appendices arise from the colon | 2 (2) |
| Unclassified | 6 (5) |
CW, Cave Wallbridge.
*Percentage of all reported cases including unclassified cases, not including this case.
Appendiceal duplication may be asymptomatic and diagnosed incidentally. However, a double appendix may cause symptoms due to inflammation of one or both appendices. Types B1 and C may be associated with congenital malformations in the large intestine and genitourinary system [4].
In this case we presented a female patient with acute abdominal pain diagnosed with acute appendicitis. In the emergency department at our hospital, patients with acute abdominal pain routinely undergo abdominal ultrasonography. The ultrasound detected an inflamed appendix but did not show the second appendix. Intraoperatively, we resected the two appendices lying on either side of the ileocecal valve. Based on the Cave Wallbridge classification our patient had type B1 appendiceal duplication. Although this type may be associated with other congenital abnormalities [4], our patient did not have any other anomalies. The diagnosis of appendiceal duplication is only confirmed when both specimens (including their tips) show an intact appendiceal structure [10]. This was confirmed in our patient histopathologically. To the best of our knowledge this case is the first to be reported in Syria.
Although appendiceal duplication is rare, it represents a challenging clinical scenario that may lead to serious ethical and legal issues if not recognized. Surgeons should always be aware of this possibility and should always inspect the cecal area carefully. In addition, acute appendicitis should always be considered in the differential diagnosis of acute abdominal pain even in a patient with a history of a previous appendectomy. Some authors feel that it is necessary to resect the duplex appendix to avoid future diagnostic confusion [4].
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}