





Abstract
Colonoscopic polypectomy reduces the risk of colon cancer development by interrupting the adenoma to carcinoma progression. A variety of techniques are available to perform polypectomy including the use of forceps or snare device with or without electrocautery. While forceps polypectomy tends to be the procedure of choice for small polyps, snare polypectomy has been found to be the preferred method for removal of polyps 1 cm or greater in size. The two most common post-polypectomy complications are bleeding and perforation. Though rare in the case of polypectomy, any mechanical device used in a procedure has an inherent risk of malfunction. Here, we present a case of an attempted snare polypectomy with malfunctioning of the device, failure of endoscopic retrieval and subsequent management with laparoscopic resection of the affected segment.
INTRODUCTION
Polypectomy is a fundamental skill required to perform effective colonoscopy screening. Colorectal cancer incidence may be reduced through polypectomy by interrupting polyp to cancer progression [1]. Multiple techniques for endoscopic removal of polyps exist with different endoscopists preferring different mechanisms of performing a polypectomy. Decisions about how to perform a polypectomy are often made at the time of colonoscopy based on the size and pedunculated or sessile nature of the polyp. Cold or hot forceps are often used for removal of small polyps <1 cm while snare polypectomy is used more frequently for polyps larger than 1 cm [2]. Special devices and advanced techniques beyond snare polypectomy for endoscopic removal of polyps have continued to develop which has decreased the number of surgical interventions needed for endoscopically unresectable polyps. Though there are established benefits of colonoscopy for detection and removal of polyps, the procedure is not without risks. Bleeding and perforation are the most common and widely recognized complications after polypectomy and occur in 1.64/1000 and 0.85/1000, respectively [3]. With the use of any mechanical device in an invasive procedure there is an inherent risk of device malfunction. Complications resulting from the malfunction of polypectomy instruments, specifically the snare polypectomy, during colonoscopy are not widely reported in the literature. Knowing how to manage complications, including malfunction of utilized equipment, is a crucial aspect of performing any procedure on patients.
CASE DESCRIPTION
A 36-year-old man underwent colonoscopy for new onset rectal bleeding, anemia, and a family history of colon cancer in his paternal grandfather as well as colon polyps in his father. On endoscopy he was noted to have nine large pedunculated polyps all >1 cm. Eight of these polyps were successfully removed with snare polypectomy. The final polyp was 3 cm located ~30 cm from the anal verge. A snare polypectomy was attempted but the snare became entrapped due to a malfunction of the releasing mechanism. The snare device was cut at the handle and a second snare was attempted to remove the polyp in a piecemeal fashion. Due to the size of the polyp limiting endoscopic resectability as well as concerns for ongoing bleeding, the patient was referred for a laparoscopic sigmoid colectomy.
During transport of the patient from the outpatient endoscopy center to the operating room the tail of the cut snare recoiled into the colon and was no longer seen when performing proctoscopy prior to the procedure. Laparoscopic ports were placed and after the abdomen was insufflated, the wire was clearly seen taking a sharp turn superior to the rectum as if it had been bent. The colon was mobilized and high ligation was performed as pathology of the polyp was unknown at the time of the operation. The bowel was then transected at the proximal rectum with a 60 mm green load powered Echelon stapler (Fig. 1). The blade of the stapler appeared to push the wire to the end of the staple line which forced the wire out of the distal rectum but did not transect the wire (Fig. 2). There was remaining adherent mesentery which was dissected away from the wire with scissors (Fig. 3). The bowel was inspected and the snare was seen exiting the proximal bowel staple line and entering the abdominal cavity (Fig. 4) with a bend on the segment of wire that was pushed to the end of the staple line with the Echelon powered stapler (Fig. 5). To assure there was no wire retained in the distal bowel a flexible sigmoidoscopy was performed prior to creating an end to end stapled anastomosis. Postoperatively the patient did well. He was discharged postoperative Day 2 tolerating a soft diet and having bowel function. His final pathology revealed a 3.4 × 3.2 × 2.7 cm3 tubulovillous adenoma with intramucosal high grade dysplasia, no evidence of invasive carcinoma and fourteen benign lymph nodes.
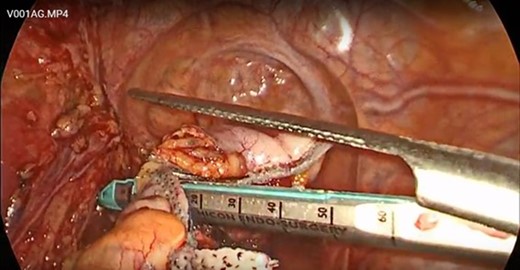
The bowel was transected with the Echelon powered stapler.
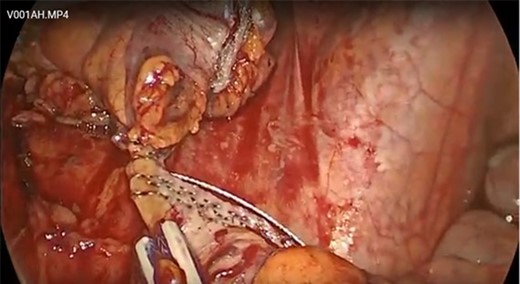
The wire was pushed to the end of the bowel but not transected.
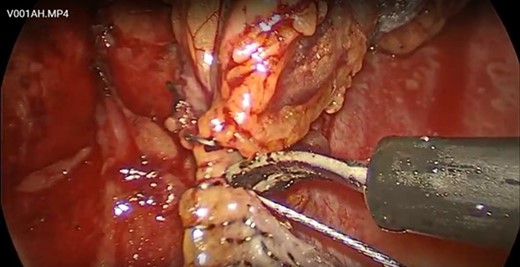
Adherent mesentery was dissected free from the snare wire.
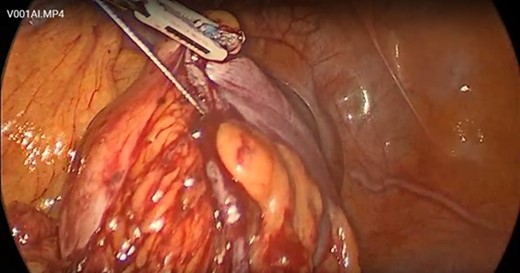
The snare wire was seen exiting the proximal bowel staple line.

There was a bend in the wire due to the stapler blade but no transection.
DISCUSSION
Though rare, snare entrapment during colonoscopy polypectomy can occur. The entrapment is often due to a malfunction in the releasing mechanism of the device as was demonstrated in our case. When this occurs a few methods of management have been described in the rare case reports discussed in the literature. These methods include removing the polyp in piecemeal fashion around the snare until the loop loosens and can be retrieved, using a second snare to transect below the first snare, or removing the polyp using endoscopic mucosal resection techniques. Not all endoscopy centers and endoscopists are prepared to utilize these techniques and more importantly, not all of these attempts are successful [4]. This results in a dilemma concerning the best operative management. Our laparoscopic management of snare entrapment demonstrates that surgery, specifically use of the powered Echelon endoscopic stapler, is an effective means of transecting bowel when endoscopic retrieval of a retained snare cannot be achieved.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}