





Abstract
Handlebar hernias are very rare and occur after a blunt abdominal trauma by a bicycle handlebar or a handlebar-shape object. As a result the abdominal wall musculature and fascia are disrupted while the skin is still intact. A good history of the injury and physical examination are usually enough to pose a diagnosis. We report the case of bicycle-handlebar hernia in a 6-year-old boy who presented to our emergency department because of a reducible swelling above the left iliac crest after falling from his bicycle 3 days ago. The patient was treated conservatively with a weekly follow-up. Four weeks later the muscle disruption was healed. In pediatric patient in the absence of internal organ injuries, a handlebar hernia can successfully be managed conservatively.
INTRODUCTION
Traumatic abdominal wall hernia (TAWH) is a rare entity caused by a blunt trauma, that has as a result the disruption of the abdominal wall musculature and fascia while the skin is intact. Handlebar hernia (HH) is a more localized type of TAWH caused by bicycle handlebar or a handlebar-shape object. There are 46 cases [1–7] reported in the literature that are related to children. In most cases, despite the absence of internal organ injuries, the treatment was surgical. We report a case of HH in a 6-year-old boy treated conservatively. The literature involving HH’s management is reviewed.
CASE REPORT
A 6-year-old boy was admitted to the emergency department 3 days after a bicycle accident. The handlebar of his bicycle traumatized his abdominal wall above the left iliac crest. Twelve hours before the admission he noticed a palpable mass and a minor bruising to this specific point (Fig. 1).

Photograph of the 6-year-old boy at the time of admission, showing the swelling above the left iliac crest.
The physical examination revealed the presence of a painless swelling measuring 8 × 3 cm2 and did not reveal any pathological sign from the abdomen. The swelling was reducible, disappeared in supine position and increased by coughing. The diagnosis of a HH was suspected and confirmed by ultrasound that showed the disruption of internal and external oblique and transverse muscle (6 × 1.5 cm2) and the projection of omentum through the hernia without other associated internal organ injuries (Fig. 2). The hematological and biochemical tests were normal. We suggested the admission of the child in our clinic for further clinical monitoring but the parents denied.
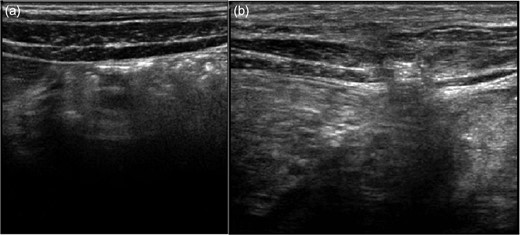
Ultrasound images of the right (a) and left (b) side of the abdominal wall at the time of admission. Left side: disruption of internal and external oblique and transverse muscles and projection of omentum.
The reassessment after 2 weeks of rest at home showed an obvious size reduction of the hernia. Because of the significant size difference a MRI evaluation was decided, that confirmed that the disruption size was 3 × 0.7 cm2. In the follow up a month later, the hernia was no longer palpable and the ultrasonography identified a defect <2 mm without herniation.
DISCUSSION
The proposed diagnostic criteria for TAWH are the history of abdominal trauma and the absence of hernia prior to trauma [8]. The feature of TAWH is the disruption of the abdominal wall musculature, fascia and peritoneum, without penetration of the overlying skin because it is more elastic.
The classification system used in children, proposed by Wood et al. [9], identify three categories of TAWH according to the amount of energy involved and the size of the hernia:
Type I: is the most common (35%) [4] and includes small defects caused by blunt trauma with objects such as a bicycle handlebar.
Type II: includes larger defects caused by high-energy trauma such as motorbike/motor vehicle accidents or falls from height.
Type III: includes defects that involve intra-abdominal bowel herniation caused by decelerating forces.
The term ‘Handlebar Hernia’ was first introduced for Type I TAWH by Dimyan et al. in 1980 as bicycle handlebar is the most common cause of this trauma [10].
Searching the English literature, 46 cases of HH in children aged 3–14 years old (mean: 9.4 y.o.) are reported since 1956. The most of them (90.4%) are boys. The location in children varies, occurring mostly in the lower abdomen: right lower quadrant: 19 cases, left lower quadrant: nine cases, left upper quadrant: three cases, right upper quadrant: one case, rectus abdominis: two cases and one in symphysis pubis—in 11 cases the location of the HH is not defined [1–7]. In our case, the hernia is located on the left lateral abdominal wall above the iliac crest.
A history of blunt trauma to the abdomen accompanied by bruising around the affected area with a visible imprint and a tender swelling, which is often reducible, with a cough impulse, should alert the physician to the possibility of a HH. The rest of the abdominal examination is usually normal. The presence of a handlebar imprint on the abdominal wall, especially at the upper quadrant, confers increased risk of associated significant abdominal injury. The cases with associated injuries of the internal organs is <20% (9 of the 47 cases). Classical signs of hernia are seen in only 50% of cases. There are cases of patients in which symptoms presented 48 h after the accident [3]. In our case the hernia was noticed 60 h after the accident.
The diagnosis of HH is mostly clinical [2]. Ultrasound has been reported as useful to confirm the diagnosis of HH and also to assess injury to solid intra-abdominal organs. Computed tomography (CT) is able to delineate the anatomy of the defect, differentiate an abdominal wall hematoma and also evaluate associated intra-abdominal injuries, especially in the case of supraumbilical injuries. Because of the radiation of the CT and the speciality on musculature, we evaluated the size of the disrupted muscles by MRI with excellent imaging results.
Management recommendation by most of the reports in the literature for HH is early or delayed surgical—open or laparoscopy—repair of the hernia to prevent complications like incarceration or strangulation [2, 3, 5, 6]. However, since 2007 several surgeons were successful in managing TAWH conservatively [1, 4, 7].
Conservative approach was used in seven cases, including our case. The defect size was up to three centimeters and the hernia contained in three cases omentum and in four cases bowel loops without incarceration. Spontaneous healing of the musculature and fascia defect was achieved in all patients in 1–12 months (mean, 4.4 months) without any complications [7].
In conclusion, in the absence of associated intra-abdominal injuries, a conservative management of HH is recommended. The small size of the defect with an absence of herniating bowel loops is an important factor in favor of conservative management. Although, is difficult to draw any firm conclusion on the basis of one case we propose that the management of children with HH must be undertaken on a case-by-case basis.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}