





Abstract
A 25-year-old male Syrian refugee presented in our hospital with recurrent hip infections after having undergone hip arthroplasty abroad following destruction of his right hip joint by shell splinters in the Syrian civil war. The patient underwent hip arthroplasty revision with implantation of a cement spacer. CT-scan with rectal contrast media filling revealed a recto-acetabular fistula. Consecutively, the patient underwent ileostomy formation. The fistula was then successfully closed by endoscopic over-the-scope clipping (OTSC®). Fistulas between intestines and joints rarely develop and in the few cases published mostly extensive abdominal rescue surgery has been performed. Here, we present a case of a traumatic recto-acetabular fistula that was successfully closed by OTSC. This innovative method could represent a safe and suitable option to effectively close fistulas between joints and intestines thereby avoiding extensive rescue surgery with bowel resection or permanent ostomy.
INTRODUCTION
In the past mass migration, the city of Munich has seen Germany’s largest influx of refugees with over 20 000 people arriving on single weekends [1]. Among these unusual health problems, we present the exceptional case of a young Syrian refugee with a traumatic recto-acetabular fistula caused by shell splinters in the Syrian civil war which was successfully and inter-disciplinary treated in our center.
Fistulas between intestines and joints rarely develop. Few cases are known to have developed both from pathologies of the hip joint [2, 3] and from anomalies of the visceral organs themselves [4, 5]. In the latter case, they often represent rare sequelae of an underlying inflammatory or malignant gastrointestinal disorder [2]. For treatment of the abovementioned fistulas, mostly extensive abdominal rescue surgery was performed. The over-the-scope-clip system (OTSC®) could represent a safe and suitable option to effectively close fistulas between joints and intestines thereby avoiding extensive rescue surgery with bowel resection or permanent ostomy. To the best of our knowledge, we report the first case of a probably traumatic recto-acetabular fistula that was successfully closed by endoscopic over-the-scope clipping (OTSC®).
CASE REPORT
A 25-year-old male Syrian refugee presented in our hospital with right-sided recurrent hip infections after hip arthroplasty which he had received in Turkey after being injured by shell splinters and gun shots during combats in the Syrian civil war. Following his treatment in Turkey, the patient had managed to undertake the wearing journey to Germany, and he got lodged in a refugee accommodation in Munich. At our institution, the patient underwent hip arthroplasty revision with implantation of an antibiotic-impregnated cement spacer in terms of a girdlestone arthroplasty. Microbiologically, an infection of the hip joint with gram-negative bacteria (Escherichia coli) and anaerobes (Solobacterium soolei, Bacteroides ovatus, Bacteroides vulgatus) was detected. Because of this suspicious spectrum of bacteria, a CT-scan (Fig. 1a) with rectal contrast media (red arrow) was performed and did reveal a recto-acetabular fistula (white arrows). As a consequence, the patient underwent loop ileostomy formation to control the feculent fistulous discharge. Consecutively, the fistula was successfully closed by endoscopic over-the-scope clipping (OTSC®, clip 14/6 t, Ovesco, Tübingen, Germany; Fig. 1b and c). After three months, the stoma could be successfully reversed after endoscopic and radiological control had been found to be without any signs of recurrent fistula, rectal stenosis or necrosis. The clip had been found to be still in situ. Afterwards, definitive hip arthroplasty was performed after negative microbiological test results. Consecutively, the patient successfully underwent rehabilitation measures.
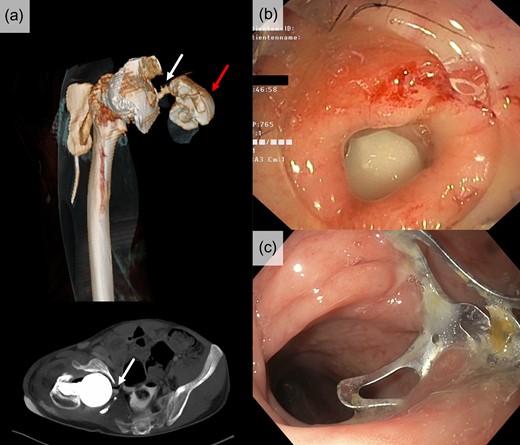
(a) CT-scan including a 3D-reconstruction (upper image) with rectal contrast media (red arrow) revealed a recto-acetabular fistula (white arrows). (b) Endoscopic view on the fistula prior over-the-scope clipping (OTSC®). (c) Successfully closed fistula with a 14/6 t OTSC® clip in situ.
DISCUSSION
The present case of a Syrian refugee with a recto-acetabular fistula and its successful minimally invasive treatment is characterized by two interesting aspects. First, it reflects the complex issues of war refugees that Munich’s hospitals are increasingly dealing with in these days. Second, to our knowledge, this is the first report of an endoscopic closure of a recto-acetabular by over-the-scope clipping (OTSC®) thereby preventing the patient from extensive rescue surgery.
War refugees from Syria suffering from physical trauma are mainly male, and a penetrating trauma (e.g. gun shots, shell splinters) is mainly responsible for the lesions [6]. In a retrospective analysis, the most frequent emergency procedures were external fixators and laparotomies [6]. In countries where refugees look for asylum, however, definitive therapies seem to become increasingly complex and expensive. However, successful management of these issues thereby providing a new perspective for refugees encourages transferring knowledge, ability and innovative visions into practice.
As mentioned above, only few fistulas between intestines and joints have been reported so far and most of these patients underwent transabdominal surgery with resection. Fistulas are known to have developed in pathologies of the gastrointestinal tract such as Crohn’s disease, diverticular disease or colorectal carcinoma treated by radiation and low anterior resection [4, 5, 7, 8]. They are also known to have spread onto the hip joint by inadequately treated anal fistula [9]. Nevertheless, hip joint anomalies can cause colonic fistulas, too. Cases are reported following girdlestone arthroplasty after necrotizing fasciitis due to cutaneous abscesses in a patient with intravenous drug abuse [2]. Most of these patients have been treated be resection of the fistulising intestinal tract, however, to the best of our knowledge, a successful application of endoscopic minimally invasive techniques with over-the-scope clipping has not been reported.
Over the past years, the endoscopic over-the-scope-clip system (OTSC®) made up of nitinol alloy has shown reliable and safe results for endoscopic treatment of acute bleeding or full thickness wall closures [10–12], the OTSC clip can grasp more tissue than standard endoclips since it is bigger and mounted on the tip of the flexible endoscope. With its high-grade elasticity, further advantages include a higher stability at the lesion site and less damage to the surrounding tissue. In addition, it can be fired off without restricting the use of the working channel. In the meantime, a wide spectrum of indications has been reported, especially regarding closure of gastrointestinal fistulas. Among these, colonic fistula caused by necrotizing pancreatitis, fistulas between gastrointestinal and respiratory tract as well as anal, anorectal and rectal fistulas were shown to be effectively treatable by OTSC clips. By closure of a recto-acetabular fistula, we were now able to present another rare possible indication with a positive outcome preventing the patient from surgery.
INFORMED CONSENT
Written informed consent was obtained from the patient prior publication of this report.
CONFLICTS OF INTEREST
The authors declare no conflicts of interest.
FINANCIAL SUPPORT
No funding was received for the present study.

{kind=link}