





Abstract
The incidence of Meckel’s diverticulum is 2% in the general population. Although most commonly found in children as painless rectal bleeding, in adults, obstruction, inflammation, and perforation are the usual manifestations. We present the case of a 32 year old man who arrived at our institution with hematochezia and symptomatic anemia. A large Meckel’s diverticulum was encountered during work-up and treated by segmental small bowel resection. A literature review, including disease presentation, pathology findings, and treatment options is discussed.
Introduction
Meckel’s diverticula represent the most frequent congenital anomaly of the gastrointestinal tract with a reported prevalence of approximately 2% in the general population [1]. It is a remnant of the vitelline duct located on the antimesenteric border of the ileum, usually within 60 cm of the terminal ileum. The structure normally regresses between the fifth and seventh week of the fetal life [2]. A Meckel’s diverticulum contains all three intestinal layers and maintains a separate blood supply from the viteline artery [2]. It is asymptomatic in the majority of cases [2]. As a congenital variant, Meckel’s diverticula are often found in children and, less commonly, present in the adult population [3]. Complications associated to a Meckel’s diverticulum include bleeding, obstruction, inflammation, and rarely, perforation. Although complications from a Meckel’s diverticulum are not usually seen in the adult population, when observed, emergency surgery is often required. We report an interesting case of a large Meckel’s diverticulum in an adult patient with an atypical presentation.
Case Report
A previously healthy 32 year old male was admitted to the emergency department at our institution, due to hematochezia of 3 days of duration, anorexia, light headedness, and fatigue. There was no history of melena, constipation, trauma or sick contacts. On physical exam the patient was hemodynamically unstable, tachycardic and pale, with a hemoglobin level of 5.2 g/dL. The patient was transfused and medically optimized. No evidence of active bleeding was noted on physical exam, or colonoscopy. A Meckel scan was found to be positive.
The patient was taken to the operative room for appendectomy, diverticulum resection, enterectomy with side to side stapled anastomosis. A 5.3 cm in length × 2.5 × 1.4 cm Meckel’s diverticulum was resected (Figs 1 and 2), along with 4.5 cm of small bowel and appendix. The patient clinical recovery was uneventful and was discharge home 3 days later.

Resected Meckel’s Diverticulum.
Discussion
Incidence rate of complications due to Meckel’s diverticulum range from 4–16% [1]. The largest study, by Yamaguchi and colleagues, 14 with 600 patients, 287 of whom were symptomatic, showed the following complication rates: obstruction, 36.5%; intussusception, which often presents as obstruction, 13.7%; inflammation or diverticulitis and perforation, 12.7% and 7.3%, respectively; hemorrhage, 11.8%; neoplasm, 3.2%; and fistula, 1.7%.

Meckel’s Diverticulum.
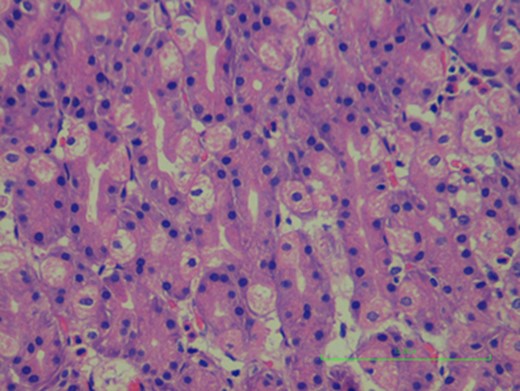
Gastric mucosa in Meckel’s diverticulum, no signs of ulceration where found.
Obstruction due to intussusception or adhesions, ulceration and inflammation (diverticulitis) are complications occurring more frequently among adults [1] (Fig. 3). Bleeding from Meckel’s diverticulum due to ectopic gastric mucosa is the most common clinical presentation, especially in younger patients, but it is rare in the adult population [1]. It is usually painless, which can be slow or even massive, manifesting as anemia or fresh bloody stools. The mechanism of hemorrhage is the ulceration caused by the acid or enzymes secreted from the ectopic digestive mucosa [4]. Intestinal obstruction is the most common complication in adult patients, with incidence rates varying from 22% to just over 50% [3]. The series by Yamaguchi and colleagues, 14 which comprised nearly 50% adults, showed hemorrhage as being less common than obstruction at a rate of almost 5:1 (54%:12%) [3].
This is a special case of Meckel’s diverticulum in adults, as the most common initial presentation is obstruction and in this case report the patient presented with painless rectal bleeding. In adults, hemorrhage occurs often but is the presenting complaint in only 11.8% [3]. Children often present with dark red or maroon stools or stools with blood or mucus, whereas adults usually present with melena and crampy abdominal pain [3]. In this case report the patient presented with painless bright red per rectum, making it a very atypical presentation for an adult. Due to the rarity of cases in adults, it is still misdiagnosed preoperatively—although with the wide spread use of technetium-99m pertechnate scan and diagnostic laparoscopic approach, the rates of preoperative diagnosis have improved [1].
Complications associated with Meckel’s diverticula tend to decrease with increasing age; a true diverticulum is rarely discovered in the adult [5]. Preoperative diagnosis of Meckel’s diverticulum is a challenge despite the availability of modern imaging. Hence, a diagnosis of symptomatic Meckel’s diverticulum demands a high degree of suspicion, as an accurate preoperative clinical diagnosis is often difficult to make.
CONFLICT OF INTEREST STATEMENT
None Declared

{kind=link}
{kind=link}
{kind=link}