





Abstract
Extra-adrenal myelolipomas (EAMLs) are extremely rare soft tissue tumours that constitute <15% of all myelolipomas. We present a 70-year-old patient with a midline swelling of the anterior abdominal wall. It was clinically diagnosed as an incisional hernia, though the computerized scan indicated an internal hernia. During laparoscopy a soft tissue tumour of the abdominal wall was identified and excised. Pathology confirmed an extra-adrenal myelolipoma of the anterior abdominal wall through the presence of adipocytes and trilineage haematopoetic cell lines. EAMLs are rare mesenchymal soft tissue tumours with less than a hundred cases reported in the English literature. Pathological diagnosis shows the presence of mature adipocytes as well as myeloid and erythroid cell lines. This is the first case report of an EAML of the anterior abdominal wall. This case report is made even more rare as it is present in a male patient.
CASE REPORT
A 70-year-old male patient presented to our institute with a midline abdominal swelling of ~6 month’s duration, clinically palpable over his epigastric region. He had no abdominal pain and the mass appeared to be increasing in size causing him discomfort. There was no history of trauma and the swelling appeared to be an incisional hernia, clinically replete with a positive cough impulse. He had a previous open mesh herniorrhaphy in the same area over a decade earlier. He had no other herniae clinically on his abdominal wall or his groin.
His medical history was significant for hypertension and alchoholism and both were well controlled. Radiological imaging included a computerized tomography (CT) scan which reported an internal hernia in the epigastrium (Figs 1 and 2). There were no radiological signs of bowel strangulation.
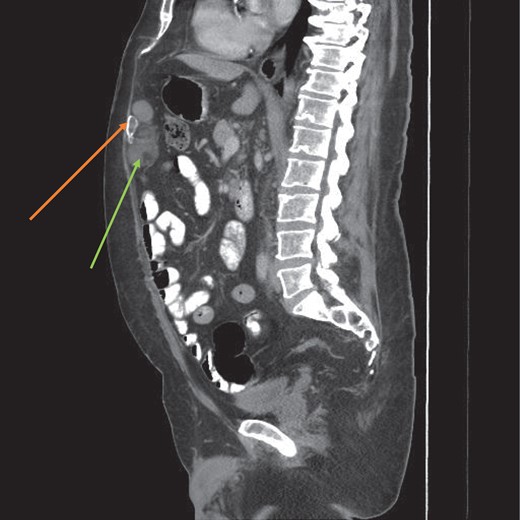
CT scan sagittal view of the myelolipoma (green arrow) with a calcified component (orange arrow).
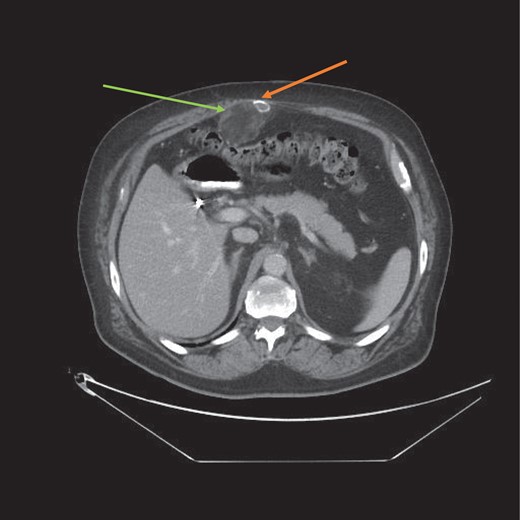
CT scan axial view of the myelolipoma (green arrow) with calcification (orange arrow). Abdominal wall musculature is intact thereby excluding an incisional hernia.
After an extensive discussion with the patient and his wife he agreed to a diagnostic laparoscopy with a view to reducing the hernia and repairing the mesenteric defect. Intra-operatively there was no internal hernia. A mass was seen in the epigastrium on the anterior abdominal wall (Fig. 3). The lesion could not be mobilized laparoscopically so the decision was made to convert to a laparotomy (Fig. 4). The lesion in the anterior abdominal wall was then mobilized and excised.
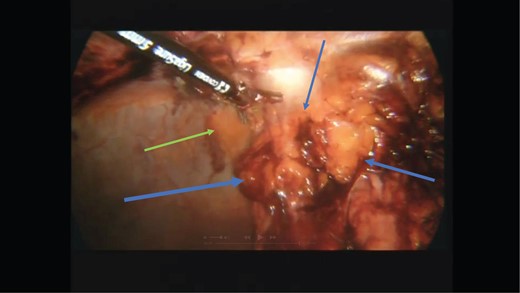
Laparoscopic view of the lesion (blue arrows) on the anterior abdominal wall (green arrow).
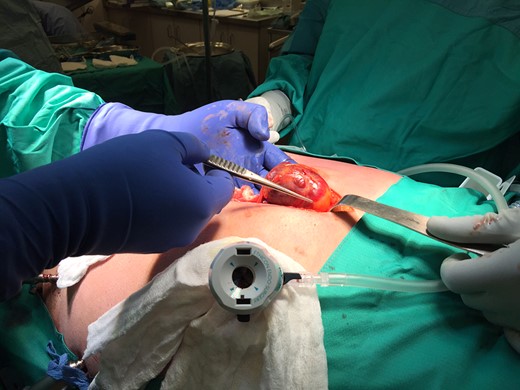
Exteriorization of the tumour at laparotomy.
Clinically it appeared to be a lipoma (Figs 5 and 6). The patient’s post-operative course was stormy with an iatrogenic small bowel perforation which necessitated a repeat laparotomy and bowel repair. He subsequently developed an aspiration pneumonia, requiring an intensive care unit (ICU) admission and total parenteral nutrition (TPN). Five days after his relaparotomy he developed a wound dehiscence that was managed with a vacuum assisted closure (VAC) device (Fig. 8).
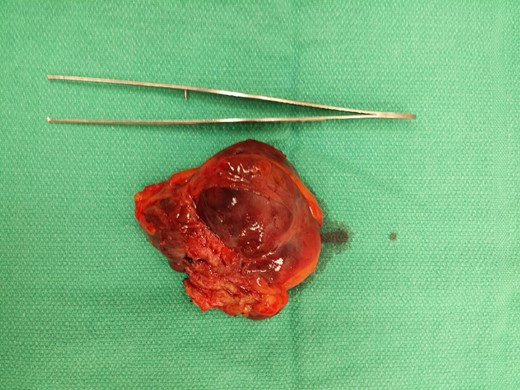
Gross pathological specimen post excision.
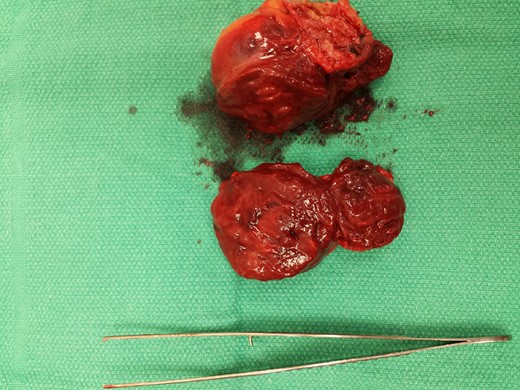
Cut section of the specimen with tumour heterogeneity.
Four weeks later he was discharged home and his VAC dressing was managed via homecare nursing.
He eventually made a complete recovery and his wound dehiscence closed 3 months later (Fig. 9). The pathology report confirmed the lesion as a myelolipoma with adipocytes and trilineage haematopoeitic cell lines (Fig. 7).
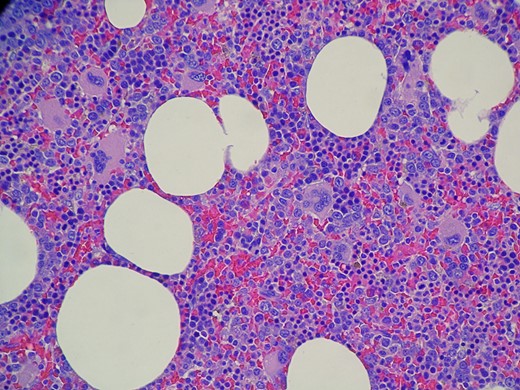
Histology slide showing the mature adipocytes and trilineage haematopoetic cell lines confirming the diagnosis of a myelolipoma.
DISCUSSION
Myelolipomas are rare mesenchymal soft tissue tumours of the abdomen and usually make up 7–15% of adrenal masses [1]. The incidence of extra-adrenal myelolipomas (EAMLs) is extremely low. EAMLs make up 14% of all myelolipomas and are usually seen in the sixth to eighth decade of life [1]. There is a female preponderance and the tumours are unilateral [2]. There have been over one hundred cases of extra-adrenal myelolipomas in the English literature to date but none have involved the anterior abdominal wall making this a truly unique presentation (Fig. 8) [3].

Post-operative wound dehiscence (blue arrow).
Treatment may entail surgical excision for symptomatic tumours [4] as they rarely display any malignant potential. Large tumours can bleed due to their haematopoeitic components so regular monitoring is essential if conservative management is considered (Fig. 9).

Complete wound healing 3 months after surgery.
The tumour consists of mature adipocytic tissue as well as haematopoeitic elements namely myeloid and erythroid cell lines. Myelolipomas were initially named by Charles Oberling in 1929, though the original tumour was first described by the German pathologist Edgar von Gierke in 1905 [5].
The aetiology of EAML remains nebulous. Two possible theories advanced include the reactivation of extramedullary haematopoetic cells or the metaplasia of adrenal cortical mesenchymal cells [6].
Based on a pubmed© and medline© search of the English literature this is the first case report of a EAML of the anterior abdominal wall. Their usual predilection is for the retroperitoneal pre-sacral space [7, 8].
This was an incidental diagnosis based on a misinterpretation of the patient’s radiological imaging. Upon further discussion with our radiology colleagues, there was a consensus view that this was indeed a soft tissue tumour of the abdominal wall and not an internal hernia as originally reported. The author himself felt that this was an incisional hernia prior to surgery based on his clinical examination and original CT findings. Diastasis recti of the rectus abdominus musculature may also have contributed to the clinical confusion of an incisional hernia (Fig. 2). Given the rarity of this tumour, a soft tissue lesion was not entertained as an initial diagnosis.
CONCLUSION
Extra adrenal myelolipomas are rare soft tissue tumours of the abdominal cavity with a female preponderance. This is the first case report in the English literature of an EAML of the anterior abdominal wall. Adding to the complexity of this case report is its presentation in a male patient which serves to reinforce the rarity of this tumour.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}