





Abstract
Extra-gastrointestinal stromal tumors (E-GIST) are group of soft tissue neoplasm, which originates from outside the gastrointestinal tract and comprises less than 5% of the total GIST. Most commonly, they originate from the omentum, mesentery, retroperitoneum or the solid organs like liver and the pancreas. E-GIST arising from the sac of the jejunal mesentery, and mimicking preoperatively as a colonic neoplasm is very rare. Here we report an interesting case of a 55-year-old male, who presented with pain abdomen for 4 months duration. Contrast enhanced computed tomography was suggestive of right colonic neoplasm. Intraoperatively, to our surprise, the tumor was seen arising from the mesentery of the jejunum and was resected.
INTRODUCTION
Extra-gastrointestinal stromal tumors (E-GIST) are the rare group of soft tissue neoplasm, which originate from outside the gastrointestinal tract. They have pathological, immunohistochemical and molecular biological characters similar to the GIST. They usually have non-specific clinical presentation and hence difficult to diagnose preoperatively. It can clinically mimic other intrabdominal disorders or neoplasm [1, 2]. Sometimes, because of the bulk of the tumor and its enhancement with the contrast on computed tomography it can mimic colonic neoplasm, such as adenocarcinoma or lymphoma. Here, we report an interesting case of a mesenteric E-GIST, which preoperatively mimicked colonic neoplasm.
CASE REPORT
A 55-year-old male, presented with pain upper abdomen, weight loss and anorexia for 4 month. The pain has increased in intensity for past 4 days, with associated malaise and vomiting. On examination, vitals were stable, with an ill-defined tender lump (7 × 8 cm) with localized guarding in the right upper quadrant of abdomen. Blood investigation showed normal hemoglobin (12.8 gm/dl), raised total leukocyte counts (14 600/mm3) and a normal liver and renal function test. Contrast enhanced computed tomography (CT) abdomen revealed an aneurysmal-like dilated, thickened and lobulated hepatic flexure of the colon with homogenous enhancement and no metastases (Fig. 1). Chest X-ray and serum carcinoembryonic antigen (CEA) level were normal. In view of change in the character of pain for the last few days, localized tenderness in the abdomen, leucocytosis and CT findings, diagnosis of right colon malignancy with localized sealed perforation was assumed, and planned for upfront (without colonoscopy and biopsy) surgery.

Contrast CT showing multiple, lobulated enhancing jejunal mesenteric GIST, which mimicked aneurysmal-like dilated (arrow), thickened hepatic flexure of colon.
Intraoperatively, to our surprise, a tumor was arising from the mesentery of the second loop of jejunum. The entire mass was present in the right upper quadrant. It was six in number, multicentric, solid, bosselated and adhered to the serosal aspect of the jejunum. Furthermore, the omentum was wrapped around the tumor, which was in fact due to the necrotic changes in one of the tumor, with impending perforation. The tumor was excised enbloc with the jejunum with macroscopically clear margin and primarily anastomosed. Cut section showed whitish-solid tumor with whorled appearances, with one tumor with necrotic changes showing tumor enteric fistula (Fig. 2). Postoperative period was straightforward and was discharged on Day 5. Pathological examination of the specimen revealed gastrointestinal stromal tumor (GIST) of the jejunal mesentery (mitotic figure—13/50 HPF, areas of necrosis suggesting high grade), which on immunohistochemistry stained strongly for CD117 and CD34 (Fig. 3). One of the dissected lymph node in the mesentery showed tumor deposits. The patient had been on imatinib 400 mg once daily for the last 6 months, and unfortunately had liver recurrence on follow-up CT scanning.

Intraoperative (A) and cut-section (B) view of solid, lobulated (arrow) and necrotic changes in the E-GIST arising from the jejunal mesentery.
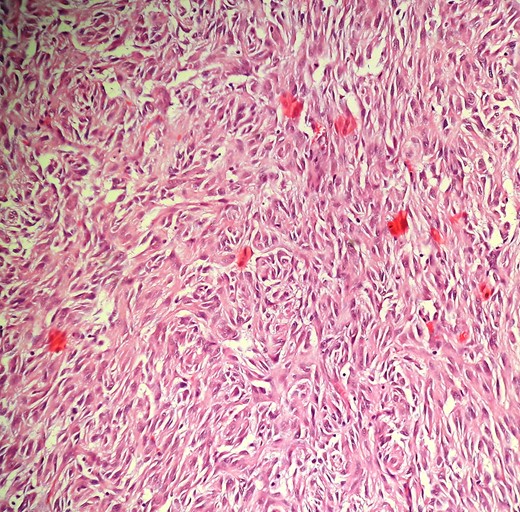
Photomicrograph (H&E,×100) showing proliferation of spindle to epitheloid tumor cells in sheets and nests.
DISCUSSION
Gastrointestinal stromal tumors (GIST) are rare neoplasm. They represent only 0.1–3% of all gastrointestinal malignancies, with the stomach (50–60%) being the most common site followed by the small intestine (20–30%), duodenum (5%) rectum (5%) and the esophagus (1%) [1]. The can rarely (5%) arise outside the GI tract as primary tumor described as extra-GISTSs (EGISTs) [2]. It was Miettinen et al., who first described this extremely rare mesenchymal tumors, which is histologically and immunophenotypically similar to GI stromal tumor. EGISTs can arise from the omentum, mesentery, retroperitoneum, liver, pancreas and prostate [3–5].
Till date, only 114 cases of mesenteric GISTs have been reported in the literature [6]. Among them only anecdotal cases of EGISTs are described to arise from the sac of jejunum [7]. Most of them presented with abdominal pain, followed by abdominal mass and distention. Unlike gastrointestinal GIST, bleeding is rarely seen [8]. Mesenteric GIST have an aggressive behavior compared to the stomach and small bowel GIST, because most tumor at presentation exceeded 10 cm in diameter (enough space to grow), exceeded 5/50 HPF in mitotic index and were high risk [6].
Establishing the diagnosis of mesenteric GIST is still challenging as these tumors donot have a specific clinical manifestations, and its rarity. Moreover, symptoms depend on the tumor size and can be observed in other GI disorders and tumor as well, as seen in our case. Contrast computed tomography shows predominantly large solid mass displacing the surrounding structures, with intense peripheral enhancement, of undetermined origin [9]. Because of the large size and the enhancement, the can mimic colonic neoplasms (lymphoma or adenocarcinoma) as seen in our patient. They are more frequently encountered during laparotomy or at receipt of pathological report for workup of abdominal lump and pain in a patient after negative upper and lower endoscopy.
The treatment consists of enbloc resection of tumor with macroscopically negative margin followed by adjuvant imatinib as almost all patients fall into high-risk category for recurrence [1, 6, 7]. Our patient had a large tumor (8 cm size), high mitotic index (13/50 HPF) with the presence of necrosis and lymph node metastases, being therefore classified high-risk EGISTs. This was the probable reason for the early liver recurrence in our case.
The 1, 3 and 5-year overall survival rates of E-GIST patients are 91.7%, 61.1% and 48.9%, respectively, which is significantly lower than that of GIST patients (with 1-, 3-, 5-year overall survival rates of 94.0%, 88.1% and 82.4%, respectively) [4]. The explanation for the significant differences in survival might be related to large tumor size at presentation and lack of gastrointestinal bleeding as seen with GIST leading to early presentations [6, 7].
In conclusion, mesenteric EGISTs, being a rare entity, can clinically mimic colonic malignancy, and can present as an acute abdomen due to the tumor necrosis. In patients with short duration history, large and well-defined enhancing abdominal mass, with normal hemoglobin and tumor marker, one should keep the possibility of mesenteric EGISTs.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}