





Abstract
Principles of type A aortic dissection surgery emphasize the importance of operative survival and long-term outcome. Various surgical strategies have emerged aiming for improved freedom of reoperation but they can be technically demanding or associated with higher operative risks. We report a type A aortic dissection case with extension of the dissection to the proximal descending aorta where a re-entry intimal tear was identified. Instead of extensive aortic arch repair, we managed the tear with a primary suture closure technique. In conjunction with a hemiarch repair of the proximal aorta, this approach enabled a prompt and complete resolution of the false lumen at minimal cost of circulatory arrest time.
INTRODUCTION
Acute type A aortic dissection (ATAAD) continues to be a challenging disease with high mortality rates in the current era. Multiple intimal entry tears frequently occur in ATAAD, which ideally should be resected or repaired in the same operative setting to prevent future aortic re-intervention. While surgical options such as a one-stage extended arch resection and endovascular repair reduce the risk of false lumen expansion and reoperation in the future, they are recommended judiciously by experts due to concerns of procedural complexity and operative risks [1, 2]. As there is no consensus on the extent of surgical repair in ATAAD, operative strategies should be individualized according to clinical scenarios [3]. Herein, we describe an ATAAD case with limited extension of dissection to the proximal descending aorta, where a re-entry intimal tear was identified and managed successfully with a primary closure technique during hypothermic circulatory arrest.
CASE REPORT
A 79-year-old man with multiple comorbidities presented with acute chest pain, and a computed tomography angiogram (CTA) showed ATAAD extending from the sinotubular junction to the proximal descending thoracic aorta with an intimal tear identified in the ascending but not distal aorta (Fig. 1). The aortic arch was not aneurysmal.
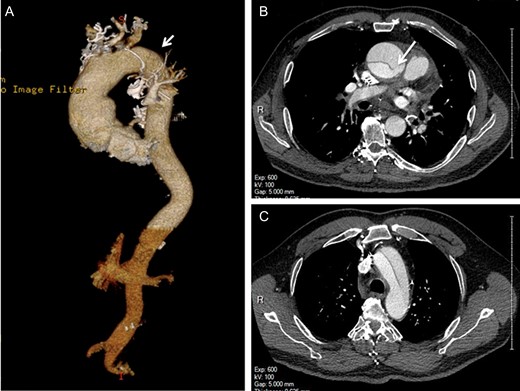
Preoperative computed tomography angiography shows the type A aortic dissection with intimal flap extending from the sinotubular junction to the proximal descending thoracic aorta (A, arrowhead). The primary entry tear is located in the ascending aorta (B, arrow). The re-entry intimal tear is not identified (C).
Emergent surgical repair was undertaken. The patient underwent right axillary artery cannulation for cardiopulmonary bypass and selective antegrade cerebral perfusion. During hypothermic circulatory arrest, a small linear intimal tear was noted at the junction of the aortic arch and the proximal descending thoracic aorta, nearly at the end of the dissection flap. Excision of the re-entry tear would require an extended total arch replacement with prolonged circulatory arrest. A frozen elephant trunk procedure was another option [4]. but it required either coverage or recanalization of the left subclavian artery since the artery was near the re-entry tear. As this was a limited ATAAD without other intimal tears identified, a decision was made to repair the re-entry tear with plegeted 4-0 prolene mattress sutures. Replacement of the ascending aorta and hemiarch was subsequently performed in the standard fashion. The circulatory arrest time was 32 min.
The post-cardiopulmonary bypass transesophageal echocardiogram confirmed the absence of flow in the false lumen (Fig. 2A). The patient had an uneventful recovery. He was discharged home on postoperative Day 6. Follow-up CTA demonstrated evolving changes in the aortic arch with complete thrombosis of the false lumen upon discharge and an interval resolution of the false lumen at 1 month (Fig. 2B and C). He remained well at 1 year postoperatively with stable appearance of the aorta on CTA.
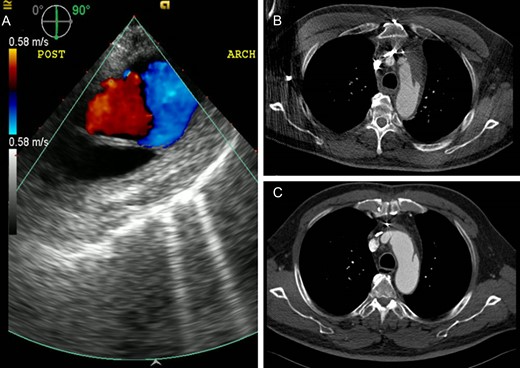
Echocardiography and computed tomography demonstrate the changes of the residual false lumen in the distal aorta. (A) Absence of blood flow in the false lumen on transesophageal echocardiography after the repair. Follow-up computed tomography scans showing interval thrombosis of the false lumen on postoperative Day 5 (B) and complete resolution of the false lumen at 1 month (C).
DISCUSSION
Most ATAADs have extension of the dissection flap beyond the aortic arch (Debakey type 1). While primary intimal tears are commonly found in the ascending aorta, it is also common to have re-entry intimal tear(s) identified in the downstream aorta. In contrast to primary entry tears that are typically extensive and require complete resection [5], distal re-entry tears can be small and subject to primary repair, promoting false lumen thrombosis and aortic remodeling.
Recent advances in surgical techniques expand the selection of surgical strategies for ATAAD. However, in certain clinical scenarios, these approaches, such as extended aortic arch repair and frozen elephant trunk procedure, may not always lead to superior outcomes. To date, hemiarch repair continues to be the mainstay approach to ATAAD [3]. In the present case, the direct closure technique served as an adjunct surgical strategy to hemiarch repair for the distal re-entry intimal tear as extensive resection and repair were less desired.
This case scenario might represent an unusual situation, as the dissection terminates in the proximal descending thoracic aorta instead of extending into the downstream aorta. The dissection flap contains a single small re-entry tear that the preoperative CTA failed to delineate. This explains why the patients had no propagation of dissection and malperfusion of the branch vessels. Our primary repair approach to the re-entry tear appeared simple and effective in facilitating aortic remodeling, thereby reducing the risk for aortic re-intervention. However, without further experience we would not generalize it as a strategy for other ATAADs with distal extensions as they are commonly associated with additional re-entry tears that can be difficult to identify. In situations where a limited repair is chosen, this approach will possibly achieve equivalent if not better outcomes and does not preclude subsequent interventions.
Surgery for ATAAD can vary depending on operative findings. Intraoperative decision-making about surgical strategies is critical. While excision of the intimal tear is still the primary strategy in the management of ATAAD, we considered direct closure of the distal re-entry tear as an option.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None declared.

{kind=link}
{kind=link}