





Abstract
Paneth cells are classified as secretory cells which are normally found in the cecum and ascending colon. Their presence in other parts of the gastrointestinal tract is regarded as abnormal and indicates metaplasia. Paneth cells may also be rarely found in gastrointestinal, biliary and prostatic tumors. The presence of Paneth cells in ovarian Krukenberg tumors is rare and to the best of our knowledge is restricted to metastatic appendiceal goblet cells tumors. We report a rare case of unilateral metastatic gastric carcinoma to the ovary in a 23-year-old female. This tumor showed unusual extensive Paneth cells metaplasia with classical signet ring cell morphology.
INTRODUCTION
Krukenberg tumor accounts for 1–2% of all ovarian tumors and is characterized by the presence of metastatic adenocarcinoma cells in both ovaries. The primary source of this adenocarcinoma could be the stomach, pancreas, appendix or other gastrointestinal sites. It is an example of a selective tumor spread most commonly in the stomach ovarian axis.
Krukenberg tumor usually shows a solid morphology with numerous signet ring mucin secreting cells which are embedded in a fibrous stroma. To the best of our knowledge, Paneth cell metaplasia (PCM) has not been described in Krukenberg tumors before, except in metastatic appendiceal goblet cell tumor [1], and for this reason our patient could represent a unique example of such an association.
CASE REPORT
A 23-year-old female patient was referred to our institution because of a history of vague abdominal pain associated with significant distension. She reported no other symptoms. Clinical examination revealed a large lower abdominal and right sided mass which was thought to be arising from the right adnexa. Full laboratory work-up showed no significant changes. Abdominal CT scan showed a large, right sided and heterogeneous adnexal mass (Fig. 1).
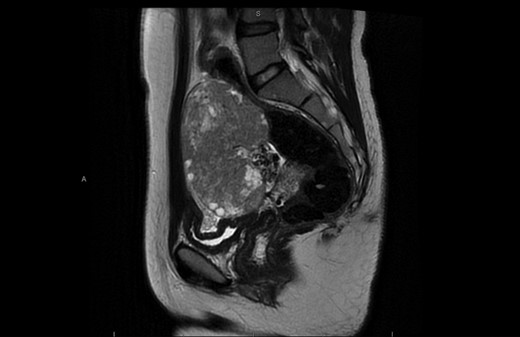
CT scan showing large right sided heterogeneous lesion 10 × 10 × 7 cm3.
The mass was later on excised and sent for histopathological assessment.
The specimen received consisted of a 10 cm maximum diameter right ovarian mass with adherent fallopian tube. On section the mass showed a predominantly solid cut surface with few small scattered cystic areas. Histopathological sections showed a poorly differentiated carcinoma consisting of a mixture of signet ring malignant cells with other cells showing granular and or eosinophilic cytoplasm consistent with PCM (Fig. 2A and B).
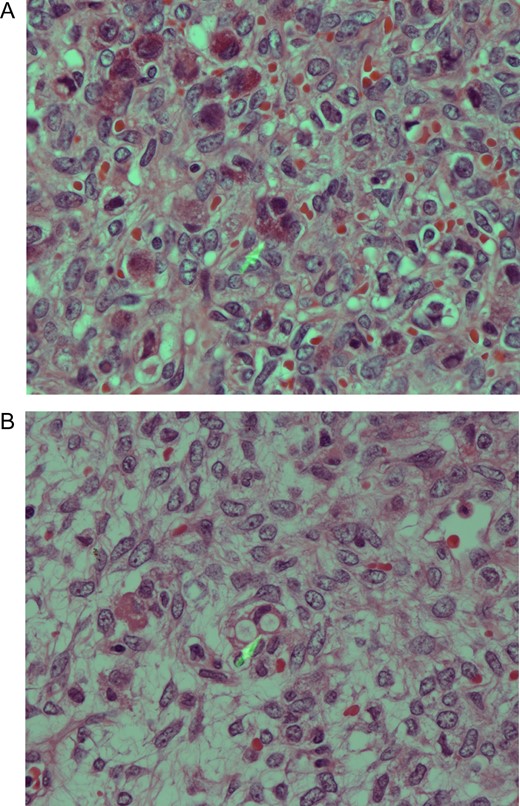
(A) Poorly differentiated carcinoma showing a mixture of vacuolated signet ring-cell malignant cells, some of which with eosinophilic cytoplasmic granules consistent with Paneth cells differentiation (PCD). H/E stain ×400. (B) Metastatic adenocarcinoma with signet ring cells morphology. Note also the presence of malignant cells containing orangophilic granules indicating PCD.
Immunohistochemical stains showed that the tumor cells were strongly positive with cytokeratin cocktail, EMA and CK7. Special stain for mucin (mucicarmine) was also positive (Fig. 3A and B).
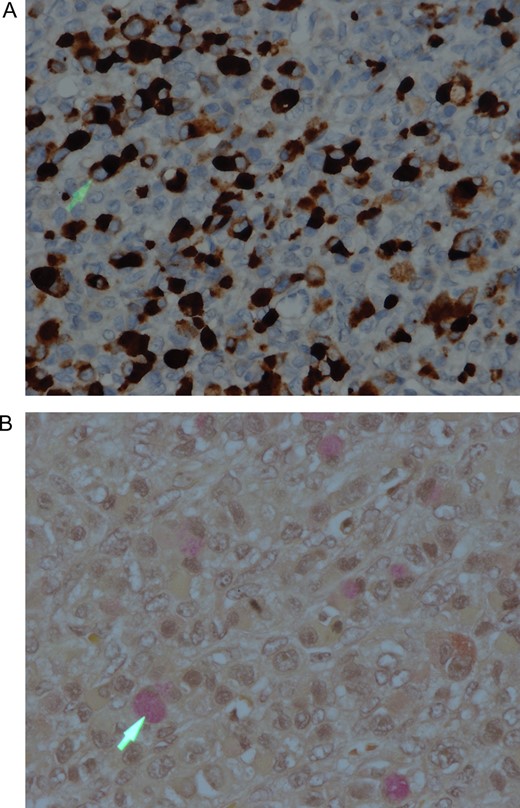
(A) Tumor cells showing strong positive cytoplasmic staining with the EMA immunohistochemistry. IHC stain ×200. (B) Tumor cells showing intracytoplasmic mucin, which is highlighted by the mucicarmine special stain (arrowhead). Mucicarmine stain ×400.
Immunohistochemical stains for lymphoma and mesenchymal malignancies were negative. A final diagnosis of metastatic adenocarcinoma with features favouring gastric origin was rendered.
A subsequent gastroscopy and biopsies were performed, and they showed a gastric adenocarcinoma of the diffuse signet ring cell subtype.
DISCUSSION
PCM is best defined as the presence of Paneth cells outside their normal site of origin which is the base of the Lieberkühn crypts of the small intestine. In the colon, a Paneth cells normally be found in the cecum and proximal parts of the colon. Their presence outside these sites in the gastrointestinal tract is regarded as pathologic and indicates metaplasia [2]. PCM is described in a variety of pathologic conditions including some neoplasms [3–6] and cases of chronic inflammatory bowel disease [7, 8].
Some authorities have found that PCM affects the prognosis of certain pre-neoplastic conditions and tumors. Furthermore, it was found by some investigators that the presence of PCM in distal colorectal adenoma is inversely associated with synchronous severely dysplastic adenoma or adenocarcinoma [9]. Chen et al. [10] also found that the presence of PCM in cases of Barrett’s esophagitis is associated with a higher risk for disease progression.
However, Kinoshita et al. [11] suggested that the presence of PCM may have anti-neoplastic and growth inhibiting effects and is hence associated with low risk of malignancy.
In general, the literature is still lacking regarding the significance and the prognosis of PCM. Needless to say, the presence of PCM in Krukenberg ovarian tumors is not clear and the impact of those cells on the prognosis of this advanced cancer needs further studies.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}