





Abstract
Although seat belts save lives after motor vehicle accidents, they may cause different types of injuries such as abdominal wall, intra-abdominal, neck and spine or vascular injuries. Seat belt sign indicates the severity of injuries, and usually the risk of intra-abdominal injuries is high when the seat belt sign exists. Here, we present two cases of intra-abdominal injuries caused by seat belts without seat belt sign.
INTRODUCTION
The seat belt sign was originally described by Garrett as ecchymosis of the abdominal wall following a motor vehicle accident [1]. This sign is accepted as an indicator of the severity of trauma and is usually associated with multiple and complex injuries. Risk of intra-abdominal injuries is high when the seat belt sign exists [2, 3]. The presence of abrasions, lacerations or ecchymosis in the seatbelt distribution warns physicians and allows the early diagnosis of injuries. However, if the seat belt sign does not exist on the patient’s body, physicians may underestimate the severity of the trauma and the patient could be discharged early without detailed clinical and radiological investigation. Here, we present two cases of the delayed diagnosis of intra-abdominal injuries caused by seat belts. Both cases had no seat belt signs or any signs of intra-abdominal injuries on presentation. We hope that our report will be beneficial for increasing the awareness of possible intra-abdominal seatbelt injuries in hemodynamically stable patients with initially negative clinical and diagnostic presentation.
CASE 1
A 22-year-old man, a passenger in the right front seat of a vehicle, was wearing a 3-point seatbelt at the time of a head-on collision traffic accident. On admission, he was conscious, his vital signs were normal, and he had no external demonstrable injuries. Abdominal tenderness was presented in initial physical examination without any other abnormal clinical or laboratory findings. An abdominal CT scan showed thickening of the small intestine wall. The patient was discharged following 5 h of stable observation in the emergency department. However, over the following 24 h, he developed a severe abdominal pain and was admitted to the emergency department. On examination, there were clear signs of peritonitis. A secondary CT scan showed free air and extensive free fluid in the abdominal cavity. During the laparotomy, a small bowel perforation 5 mm in diameter, and a large volume of intestinal fluid were detected (Fig. 1). Primary suture was performed to the perforation site. Postoperative course was uneventful and the patient was discharged on the sixth postoperative day.
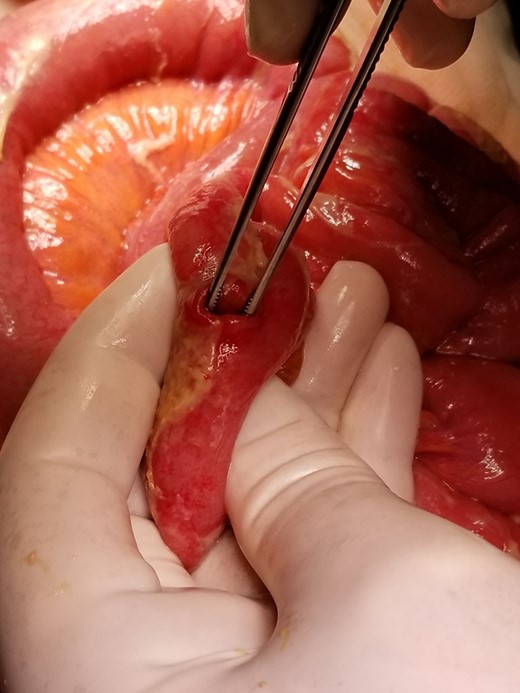
Isolated small bowel perforation, situated 100 cm proximally from the ileo-caecal valve due to seat belt.
CASE 2
A 38-year-old male driver was wearing a 3-point seat belt in head-on traffic accident at a speed of ~80 km/h. On admission, he was conscious, his vital signs were normal and he had a right knee fracture. An abdominal CT scan showed small splenic hematoma and minimal free fluid intra-abdominally. He was hospitalized and monitored for 10 h. However, his general condition gradually deteriorated, his abdominal pain increased, hypotension and tachycardia developed. A second CT scan was performed and revealed that intra-abdominal free fluid had increased, and the distal part of the small bowel was ischemic with thickened walls. During the laparotomy, there was more than 2 l of blood and hematomas, and a 100 cm small bowel mesenteric laceration starting from 10 cm above the ileo-caecal valve (Fig. 2). This bowel segment was ischemic but had no perforation. There was also laceration of the sigmoid colon and upper rectum mesocolon. A 100 cm small bowel resection and end-to-end anastomosis were performed. The postoperative course was straightforward, and he was discharged on the ninth postoperative day.
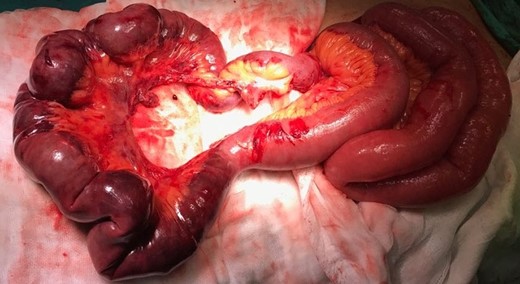
Small bowel’s mesenteric laceration starting from 10 cm above the ileo-ceacal valve. This bowel segment was ischemic but had no perforation.
DISCUSSION
The use of seat belts has significantly decreased morbidity and mortality associated with motor vehicle accidents [4]. Although the benefits of seat belts are clear, it should not be forgotten by physicians that seat belts are associated with their own patterns of injury [3]. Victims of traffic accidents wearing seat belts may experience different types of injuries, ranging from abdominal wall and intra-abdominal injuries, neck and spine injuries to chest wall trauma or vascular injuries of the abdominal aorta and supra-aortic arteries [3].
Early diagnosis of intra-abdominal injuries provides better outcomes for patients with seatbelt injuries, but this remains a challenge for trauma surgeons. The abdominal pain in polytraumatized patients may be dominated by pain resulting from extra-abdominal injuries. Delayed presentation and missed injury on radiologic investigations are the most common reasons for delayed diagnosis of intra-abdominal injuries after a motor vehicle accident [5]. Seat belts can cause some intra-abdominal injuries such as small bowel perforations, mesenteric lacerations or intra-abdominal bleeding. If the intra-abdominal injury is severe, peritonitis develops immediately and diagnosis is easy with physical examination and CT scan. However, if the intra-abdominal injury is small, such as small perforation of the bowel or small mesenteric laceration, diagnosis is very difficult. The lack of seat belt sign on the victim’s body is another important factor for delayed diagnosis. It is accepted that if the seat belt sign is not present, the risk of intra-abdominal injury is very low [6]. Physical examination of these patients is usually unremarkable on first admission and abdominal ultrasound or even CT scans might be normal. Peritonitis develops slowly in these patients and it leads to difficulties in early diagnosis. Biswas et al. [7] reported that 17.1% of their patients were diagnosed late, mostly due to delayed presentation. The reasons for late diagnosis in our cases were delayed presentation and missed injury on CT scan. Both of our cases also had no seat belt sign despite the presence of intestinal injuries. They developed severe abdominal pain and clinical deterioration during the follow up period. Therefore, the lack of this sign does not guarantee that all intra-abdominal organs are healthy, even if the CT scan is normal. If the patient has abdominal pain, physicians should be cautious about intra-abdominal injuries and follow the patients carefully. We would recommend repeated physical examinations and close monitoring, with judicious use of available imaging modalities for patients with abdominal pain after motor vehicle accidents.
CONCLUSION
We would recommend that CT scan is performed for haemodynamically stable patients with abdominal pain after a motor vehicle accident, even if there is no seat belt sign. If the CT scan is normal, the patient should be hospitalized and followed closely for up to 24 h. A control CT scan should be performed and an explorative laparotomy should be planned if peritonitis signs develop.
ACKNOWLEDGEMENTS
The authors thank Mr Simon Thompson from Near East University for language editing and proofreading.
CONFLICT OF INTEREST STATEMENT
None.

{kind=link}
{kind=link}