





Abstract
A linear stapler with bioabsorbable polyglycolic acid felt is widely used during the resection of emphysematous lung. Currently, an improved staple device with polyglycolic acid felt is being used owing to a history of complications, such as bleeding, that was associated with the previous model. Here, we report a case of a 69-year-old man who presented to our department for treatment of left lower lobe lung cancer using the new staple device. A left lower lobectomy and emphysematous bullectomy were performed. Reoperation was performed following the diagnosis of a postoperative hemothorax. During that operation, a staple with reinforcing material was found to be in contact with the proliferating vessels on the lung surface, resulting in an active bleed. The vessel was cauterized, and the bleeding stopped. This is the first case study to report bleeding associated with the improved staple device.
INTRODUCTION
The usefulness of a linear stapler with bioabsorbable polyglycolic acid (PGA) felt is recognized in every surgical field. In thoracic surgery, it is often used to prevent the formation of postoperative pulmonary fistulas in emphysema lung patients [1, 2]. In the lungs of such patients, there is frequently an increase of blood vessels on the visceral pleura and around the emphysematous bullae.
However, a linear stapler with bioabsorbable PGA felt had been recalled because there was a reported case of postoperative bleeding and a case with a fatal complication [3, 4]. Currently, the device has been improved, as it is now reinforced with a more flexible PGA sheet; its effectiveness is widely recognized, not only in the thoracic surgical field, but also in all surgical fields [1, 2]. Since these improvements, there have been no other reports of postoperative bleeding associated with its use; to our knowledge, this is the first report on postoperative bleeding relating to the reinforced staple device. Here, we describe the case of a 69-year-old man who underwent surgical treatment for left lower lobe lung cancer using a linear staple device with bioabsorbable PGA felt, which resulted in bleeding complications.
CASE REPORT
A 69-year-old man presented to our department for the treatment of left lower lobe lung cancer (adenocarcinoma, cT2aN0M0 stage IB) (Fig. 1A). He was previously a heavy smoker (Brinkman index 720); he did not take anticoagulants or antiplatelet drugs, as the coagulation tests revealed no abnormalities. Preoperative chest computed tomography revealed that pulmonary emphysema was dominant in both the upper lobes, and multiple bullae were found in the apex of the lung (Fig. 1B).
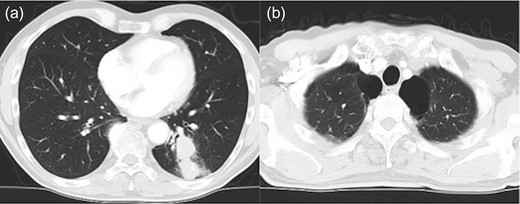
Chest computed tomography shows lung cancer in the left lower lobe of the lung (a) and an emphysematous lung with bullae in the lung apex, bilaterally (b).
Left lower lobectomy and lymph node dissection were performed. Preoperative computed tomography imaging revealed multiple bullae in the apex of the left lung and very thin bullae walls (Fig. 2A). Concerned that the patient would develop a second primary lung cancer or pneumothorax in the future, we simultaneously performed a bullectomy for two bullae with a lobectomy (Fig. 2B). Because the patient’s lung was highly emphysematous, linear staplers with PGA felt (Endo GIA™ Reinforced Reload with Tri-Staple™ Technology, cartridge color: purple, MEDTRONIC, Tokyo, Japan) were used for the bullectomy. We confirmed the absence of bleeding in the thoracic cavity and completed the operation (Video 1). The drainage from the thoracic tube turned bloody beginning 1 h after the operation. The drainage volume increased, and 600 ml of bodily drainage was observed for 2 h after the drainage had turned bloody. A chest X-ray imaging examination was performed, which confirmed fluid accumulation in the left thoracic cavity (Fig. 3). Because the patient’s anemia had also progressed, as compared with preoperative measurements (preoperative hemoglobin, 12.8 g/dl; 3-h postoperative hemoglobin, 9.1 g/dl), we determined that sustained bleeding had occurred in the thoracic cavity; we subsequently decided to carry out a reoperation to perform hemostasis. No air leakage was observed during the period between both operations.
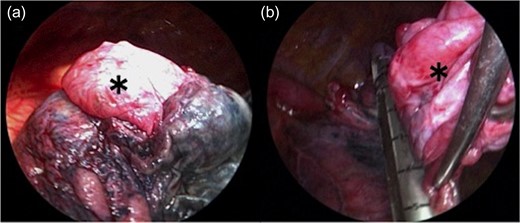
The bulla (*) wall in the apex of the lung was very thin (a). Following left lower lobectomy, the resection of emphysematous bullae (*) was performed (b).
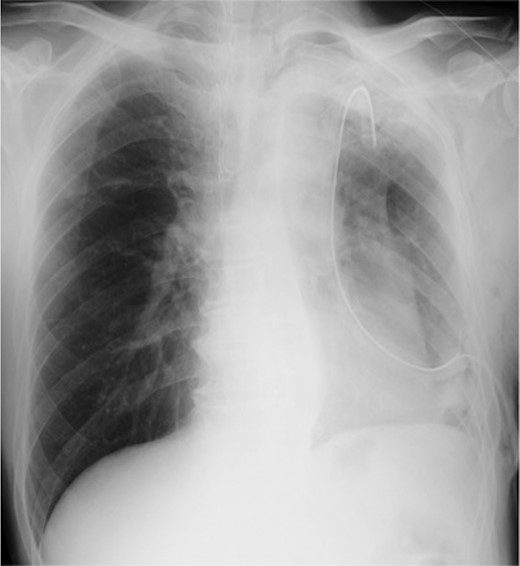
Chest X-ray image 2 h after the presence of bloody drainage from the thoracic tube caused suspicion of a left hemothorax.
During open thoracotomy, a large hematoma was observed extending from the chest apex to the mediastinum. The hematoma was removed, and we searched for the source of bleeding; there was no evidence of bleeding from the great vessels. Active bleeding was observed from the lung surface near the staple line, an area where the bullae had been resected. The bleeding source was cauterized and the bleeding stopped. Observation of the bleeding source revealed blood vessels growing on the visceral pleura and that the staples with tissue reinforcement were in contact (Videos 2, 3). A part of the staple in contact with the proliferating blood vessel was excised. We confirmed that there was no other bleeding site and completed the operation. The postoperative course was uneventful, and the patient was discharged on the eighth postoperative day.
DISCUSSION
In the case described above, postoperative bleeding was observed in a patient who had undergone surgical treatment that used a linear staple device with bioabsorbable PGA felt. Based on observation during the reoperation to perform hemostasis, we suspected that the bleeding was caused by the following mechanism. As the staple with the PGA sheet remained in the staple line with a certain length, the surplus staple made contact with the proliferating blood vessels on the lung surface. Thus, damage to the blood vessels occurred when the lungs expanded after the operation.
It is reported that the risk of developing lung cancer on the wall of an emphysematous bulla is high [5]. In this case, to reduce the risk of developing a second lung cancer or pneumothorax, we performed a bullectomy. In thoracic surgery, the primary purpose of using a linear stapler with bioabsorbable PGA felt is to prevent the formation of a lung fistula at the time of a bullectomy or resection of emphysematous lungs. In such lungs, blood vessels often increase on the visceral pleura, around the emphysematous bullae. Such a proliferating blood vessel is abundant in blood flow, and even slight damage can lead to major bleeding, as shown in this case. In this case, air leakage was not observed. The fact that no air leakage was observed suggests that pleural damage did not occur beyond the pulmonary parenchyma and only injury to the blood vessel on the pleural surface had occurred. If the intensified blood vessel remains near the staple line, the excess staple, which is integrated with tissue-reinforcement material, may come into contact with the blood vessel. In such a case, it may be appropriate to cover the lungs with PGA sheets or to remove surplus staples.
A limitation of this study is that microscopic observations could not be made because the damaged area was not resected. Within the limitations of a single case report, this case demonstrates a potential complication related to the use of the improved stapler device.
To our knowledge, this is the first report on postoperative bleeding relating to the improved staple device. When using a linear staple device with bioabsorbable PGA felt, it is important to pay attention to secondary damage of surrounding tissues, such as with large or proliferative blood vessels.
ACKNOWLEDGEMENTS
Not applicable.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no competing interests.
FUNDING
Not applicable.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
This case report was approved by the local institutional and ethics review board. Because it was not a trial, consent to participate was not required.
CONSENT FOR PUBLICATION
Written informed consent was obtained from the patient for the publication of this manuscript and all accompanying images and videos.
AVAILABILITY OF DATA AND MATERIALS
The datasets supporting the conclusions of this article are included within the article and its additional files.

{kind=link}
{kind=link}
{kind=link}