





Abstract
Complete duplication of ureters is a very rare clinical entity that may either be asymptomatic or present with a variety of clinical findings. In the presented case a 51-year-old Caucasian female underwent an intersphincteric resection for low rectal cancer. Intraoperatively, during the standard bilateral recognition and mobilization of the ureters, complete unilateral duplication of the left ureter was incidentally detected, deriving from a single renal parenchyma. Such a congenital abnormality though constitutes a major risk-factor of accidental ureteral injury during operations including pelvis. Conclusively, meticulous exposure of both ureters combined with surgeons’ unceasing awareness constitute the cornerstone of a safe operation.
INTRODUCTION
Ureteral duplication is one of the most common renal congenital abnormalities with an incidence of 0.7–4% [1]. Complete ureteral duplication constitutes the most scarce ureteral aberration that can either present bilaterally or unilaterally and represents the 33% of incomplete duplications [2]. All forms of renal duplication have a 2:1 female predominance [3].
Patients with ureteral duplication may be usually asymptomatic or they may present with a variety of clinical manifestations such as urinary stones, ureterocele, vesicoureteral reflux, urinary tract infection and obstructive uropathy [4]. Additionally, such a variation constitutes a severe risk-factor of intraoperative ureteral injury that is a potential complication of any open or laparoscopic surgical procedure involving the pelvis [5].
The present article aims to highlight the safe surgical administration of complete unilateral ureteral duplication with a single renal parenchyma that was incidentally detected during intersphincteric resection for low rectal cancer.
CASE REPORT
A 51-year-old Caucasian female presented with the diagnosis of low rectal cancer. Clinical symptoms began 4 months ago and included mild lower abdominal pain, accompanied by changes of intestinal transit and rectal hemorrhage. The patient’s medical history disclosed no evidence of urinary tract symptoms. Digital rectal examination, revealed a tumor in the posterior rectal wall. Colonoscopy showed a polypoid formation located at 4 cm from the anal orifice and the histopathological analysis demonstrated a well differentiated, Grade I, infiltrative rectal adenocarcinoma.
Additional imaging examinations such as CT of thorax, abdomen and pelvis detected no distant lung or liver metastases. The patient underwent preoperative long course chemoradiotherapy of 5-week duration and 50 Gy total dose, which was administered in 25 fractions and combined with 5-fluorouracil (5-FU), without any serious side effects. Finally, intersphincteric rectal resection with total mesorectal excision was scheduled.
Intraoperatively, during the recognition of the left ureter, which sustains a standard practice during colon and rectal surgery in our department, since reassuring avoidance of ureteral injury and subsequent complications, a complete duplication of the left ureter was incidentally detected originating from a single renal parenchyma, but draining separately into the urinary bladder (Fig. 1). No congenital abnormality of the urinary tract was identified regarding the right ureter (Figs 2 and 3).
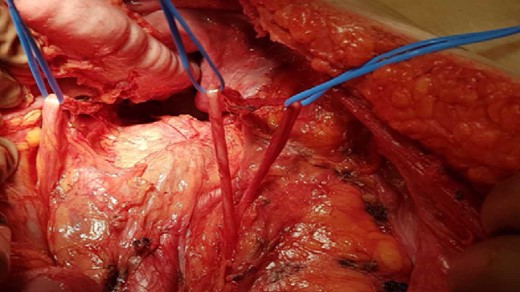
Detailed exposure of both ureters (right ureter without aberration).
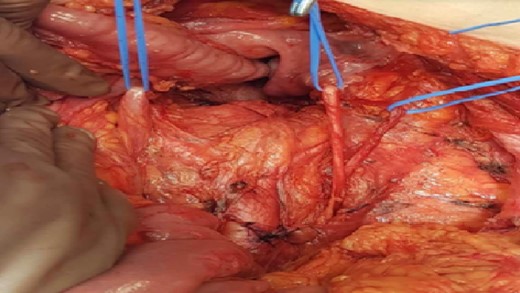
Complete unilateral ureteral duplication of the left ureter.
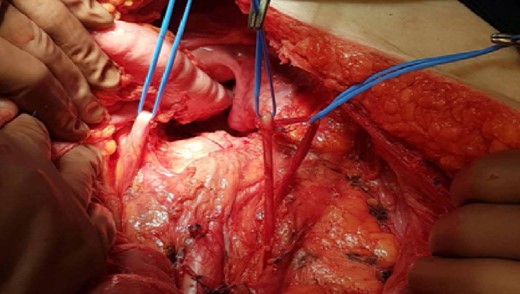
Complete unilateral ureteral duplication of the left ureter.
Then, the operation continued in the usual fashion and a hand sutured coloanal anastomosis was performed (Fig. 4). The patient recovered uneventfully and was discharged the sixth postoperative day. The patient did not present any urinary tract symptoms postoperatively and was advised to seek special urological consultation if ever needed in the future.

Performance of the hand sutured coloanal anastomosis using absorbable sutures placed in between the colon, the external sphincter and the anoderm.
DISCUSSION
Duplicated ureters deriving from a single kidney is a rare congenital anatomical variation [6] where the ureters may either join to form a partially duplicated ureter or they may remain fully separated and create a complete duplication, as in the presented case. Unilateral ureteral duplication was found in up to 0.8% in autopsy studies, while bilateral duplication was found in 0.16–0.32% [6].
Complete ureteral duplication may be embryologically explained by the development of two separate ureteral buds deriving from a single nephric duct [7]. Duplication is believed to be inherited in a autosomal dominant way, presenting with incomplete penetrance [8] and often appears in Caucasian females, as in our case [9].
Clinical manifestation of ureteral duplication is extremely variable and highly dependent on the patient’s age. Most of these cases are diagnosed prenatally with repeated episodes of urinary tract infections [9]. In adult life, this specific congenital abnormality may run asymptomatically or present with hematuria, abdominal or flank pain and predispose to obstruction, vesicoureteral reflux and recurrent urinary infections [4]. Such an abnormality though, increases the probability of ureteral injury during surgery.
In particular, ureteral injuries represent a common complication of any open or laparoscopic surgical procedure involving the pelvis, such as colorectal, general, vascular, urologic and gynecologic surgery, with the latest standing for more than half of all the above mentioned procedures [10].
The use of preoperative ureteral radiographic imaging by intravenous urography or CT has been widely advocated when encountering large pelvic masses or pelvic inflammatory disease.
Furthermore, placement of ureteral stents may be helpful as well when large pelvic tumors are expected or congenital abnormalities are suspected, although their placement is not recommended on a routine basis. Their presence fascilitates the intraoperative identification and palpation of the ureters and prevents their injury or kinking by adjacent suturing [10].
Nevertheless, neither ureteral stenting, nor preoperative imaging contrast studies may prevent ureteral injuries as efficiently as surgical awareness. Indeed, accidental ureteral injuries can be easily avoided if the surgical team emphasizes on recognizing and fully mobilizing the ureters in the specific operative field, as in the presented case.
Moreover, whenever ureteral injury is suspected intraoperatively, the surgical team must meticulously examine the area of interest, since direct exploration and visual inspection are the most safe and accurate methods for diagnosis.
Conclusively, early recognition, detailed exposure of the operative field, mobilization of both ureters and surgeon’s perpetual awareness concerning this rare urinary abnormality are the cornerstone of a safe operation when performing intersphincteric rectal resection and other surgical procedures including pelvis.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}