





Abstract
Brachymetatarsia is a rare forefoot deformity predominantly affecting the fourth metatarsal. Current treatment include gradual lengthening by distraction osteogenesis using an external fixator or single-stage lengthening with bone grafting or a combination of the above two procedures. Our aim was to assess outcomes and complications of a novel technique for gradual metatarsal lengthening using a circular fixator. The procedure was performed on three female patients with unilateral congenital shortening of the fourth ray. All participants reported aesthetic dissatisfaction as well as pressure related complications of the deformity and opted for lengthening and distraction osteogenesis using a frame. Mean duration of the treatment was 122 days and average length gained was 12 mm. The desired metatarsal length was achieved in all three patients with no significant complications. This method of treatment of brachymetatarsia is effective and reproducible. This a promising technique, owing to its low complication rates and efficacy in lengthening.
INTRODUCTION
Brachymetatarsia or one or more shortened metatarsals, is a rare forefoot deformity, reported as having an incidence of 0.02–0.05%. It is more than 25 times more prevalent in females compared to males. Most commonly, it affects the fourth metatarsal and as many as 72% of cases present bilaterally [1–3].
Brachymetatarsia is defined as one metatarsal ending 5 mm or more proximal to the parabolic arch of the other adjacent metatarsals [1, 2]. A shortened metatarsus can be congenital (Fig. 1) or acquired through trauma, infections, tumours or iatrogenic.
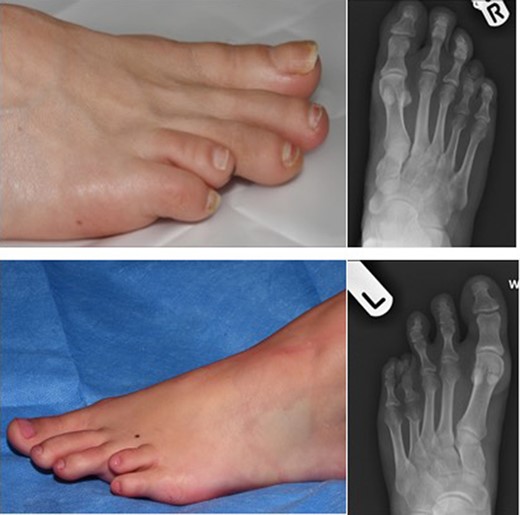
Pre-operative images on the left alongside x-rays on the right depicting congenitally short fourth toes.
Cosmetic concerns are common cause for presentation, especially in younger females, when the deformity becomes more pronounced at the end of skeletal maturity. However, it needs to be considered that several patients report irritation by footwear due to the abnormal position of the shortened toe, pain in the toes or forefoot and the development of callosities due to the abnormal distribution of plantar pressure [3].
Surgical correction of the deformity has been described to achieve increased toe length using various techniques. Most commonly used techniques include gradual lengthening by distraction ostogenesis using an external fixator or single-stage lengthening, often with bone grafting [2, 4] or a combination of the two.

Circular external fixators showing application method.
Single-stage lengthening with intercalary bone graft is well documented in literature. It offers improved patient compliance and reduced healing time [5]. In a large systematic review by Jones et al. [2], mean healing time of 9.35 (range 5–14) weeks was reported for single stage lengthening group as compared to 16.04 (range 7.3–68) weeks in the callus distraction group. Complications of single stage lengthening include neurovascular compromise and hence a reduced achievable length, bone graft resorption, MTPJ stiffness, mal-rotation of digits and metatarsal angulation [6, 7].
Gradual lengthening procedures using distraction osteogenesis is currently utilized by most surgeons. The advantages of gradual lengthening include greater achievable length, reduced time to weight bearing, preservation of movement of the MTPJs and less compromise of soft tissues when compared to single-stage surgery [3, 4].
The most common complications encountered when using a gradual lengthening technique are MTPJ stiffness, mal-alignment, subluxation and superficial skin infections from pin tracts [2, 7, 8]. The complication rates are consistently high, reportedly 59.3% according to Barbier et al. [5] when comparing results from international literature.
The majority of publications regarding gradual bone lengthening describe the use of unilateral external fixators with scant publications on the use of semi-circular external fixators [9] and none reporting the use of circular external fixators (Fig. 2).

Figure on the left showing trans-metatarsal K-wires in-situ along with the toe carrying wire cut and left alone. Figure on the right showing callus formation over distraction zone.
CASE REPORT
The aim of this prospective case series is to assess outcomes and complications of a novel technique for gradual metatarsal lengthening using a circular fixator followed by trans-metatarsal k-wire fixation. The circular external fixator applies Ilizarov principles which describes the importance of increased frame stability and thus better control of alignment and reduced subluxation [5]. The trans-metatarsal k-wires (Fig. 3), placed after removal of the external fixator, prevents further subluxation. We theorise that using a circular external fixator followed by trans-fixation metatarsal k-wires could reduce complication rates associated with distraction osteogenesis using external fixators and potentially improve the healing time along with restoration of metatarsal parabola and subsequently improving the biomechanics of the forefoot (Fig. 4).

Pre-operative image on the left with image on the right showing successful lengthening.
This study is a prospective case series of three female patients who underwent our novel distraction osteogenesis technique for congenital shortening of the fourth ray. All patients were affected by unilateral brachymetatarsia, one involving the right foot and the others the left. All participants reported aesthetic dissatisfaction as well as pressure related complications of the deformity.
Patients were offered a simple tendon release, single-stage distraction with bone grafting or lengthening and distraction osteogenesis using a frame as they were not happy with the non-operative management. The advantages of each procedure as well as predicted long term outcomes, postoperative requirements and possible complications were discussed at length. All patients opted for lengthening and distraction osteogenesis using a frame. Prior to surgery the procedure was discussed with the patients in detail and they were fully informed regarding the treatment duration, immediate and long term postoperative requirements and potential complications. Written informed consent was obtained from each patient.
The aim of the procedure was to achieve anatomic restoration of the metatarsal parabola and subsequently improved biomechanics of the forefoot and cosmesis.
Two Ilizarov rings were applied across the fourth metatarsal. Proximal ring constituted of two 1.8 mm olive wires through the tarsal bones and distal ring constituted of two 1.4 mm trans-fixation olive wires. The metaphyseal osteotomy was performed with osteotome after pre-drilling. Separate toe carrying wire was used to transfix metatarsophalangeal joint to maintain stability and to prevent subluxation. The patients were kept non-weight bearing on the operated foot until the removal of external ring fixators. Distraction was initiated in all patients after an eight-day waiting period at a rate of 1 mm/day using clicker rod turned four times a day. Radiographic evaluations were performed at 2, 4 and 6 weeks after surgery and at the last appointment.
Once the desired length was achieved through distraction, the frame was removed and replaced with transfixing k-wire and weight bearing Bootie.
All were female patients with unilateral congenital fourth metatarsal shortening causing the deformity. Mean age of the participants was 31.6 years (20, 27, 48). All patients reported aesthetic dissatisfaction as well as pressure related problems of the deformity.
External fixator removal was performed in theatre at an average of 62 days after surgery. Trans-metatarsal k-wires were placed on the same day. All of them were given Bootie and instructed to weight bear as pain allowed.
The trans-metatarsal k-wires were removed at a mean of 33 days (24–42 days) after placement. Mean time for completion of treatment was 122 days (111–127 days) and the average length gained was 12 mm (15, 14, 7 mm).
All patients achieved the desired length to fulfil the parabola of forefoot along with the cosmesis without any wound problems or secondary deformities.
DISCUSSION
Brachymetatarsia is a rare deformity which is cosmetically concerning as well as physically symptomatic. It can be an isolated problem or as part of a syndrome. Surgical treatment options include, one stage lengthening with bone graft, gradual distraction osteogenesis with or without bone grafting. Both methods has its own advantages and disadvantages.
Single stage lengthening with bone graft is associated with fewer complications and faster healing times but with lesser gain in length and hence suitable only for minor shortenings of metatarsals [2]. At the same time, distraction osteogenesis technique is associated with greater gain in length but results in higher complication rates and requires almost twice the time to heal [2]. However, this does not have issues of donor site morbidities as compared to single stage lengthening.
Our series of patients in whom we used the complete ring fixator, achieved the required length of metatarsal to address both the cosmesis as well as the mechanical problems without having any significant complications associated with the traditional uniaxial external fixators. We believe that having a ring fixator on either sides of the distraction zone, gives more control of the alignment and the flexibility to address most of the problems that might come up. It is more stable and hence there is increased callous formation and predictive distraction with less infection rates. Frame time is reduced by conversion to trans-fixation wires with frame removal. The use of complete ring fixator for this rare condition has not been reported before. However, this has to be performed by a surgeon who is trained to perform ring fixators.
We conclude that brachymetatatarsia with significant shortening can be treated by distraction osteogenesis using ring fixator followed by trans-metatarsal k-wire, without the traditional higher complications associated with external fixators. Our clinical experience so far are quite promising. However, we agree that our numbers are limited and hence this needs to be explored with higher numbers in the future.
ETHICAL APPROVAL
Ethical approval was obtained from the Hospital ethical committee.
CONSENT
Written consent obtained from each patients after detailed explanation by the surgeon.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
Author notes
The authors whose names are listed immediately below certify that they have NO affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this article.

{kind=link}
{kind=link}
{kind=link}
{kind=link}