





Abstract
Abdominal wall hernias are a rare but important consequence of blunt trauma. The optimal timing and the method of repair are not well described in the current surgical literature. Advances in laparoscopic techniques have offered new options for treatment of this problem. We describe the case of a 43-year-old man who suffered a blunt traumatic lumbar hernia. He was taken to the operating room during his initial hospitalization where a laparoscopic repair was performed with the additional implantation of prosthetic mesh. His post-operative course was uneventful. In selected cases, early operative repair may be appropriate and result in improved outcomes.
INTRODUCTION
Hernias are weaknesses in the lining of the abdominal cavity. They can occur either due to congenital or acquired conditions. When left alone, abdominal hernias can enlarge. This can result in patient discomfort or worse, intestinal incarceration and strangulation. Traumatic abdominal wall hernias are acquired conditions that have been know to occur for over 100 years with the first described report occurring in 1906 [1]. While penetrating abdominal wounds logically have a significant risk for creating trauma abdominal wall hernias. Blunt mechanisms of trauma resulting in abdominal wall hernia are uncommon, accounting for only 1% of all blunt trauma admissions [2]. The optimal timing and type of hernia repair has not been defined [3] We present the case of a patient presenting with a traumatic lumbar hernia which was repaired laparoscopically during the index hospitalization.
CASE REPORT
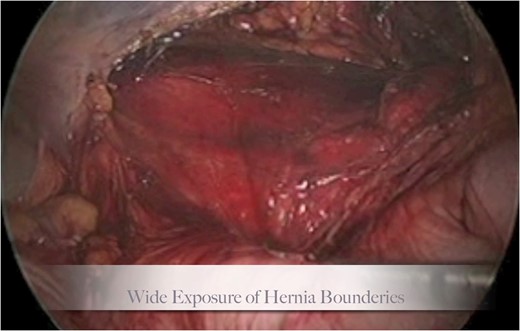
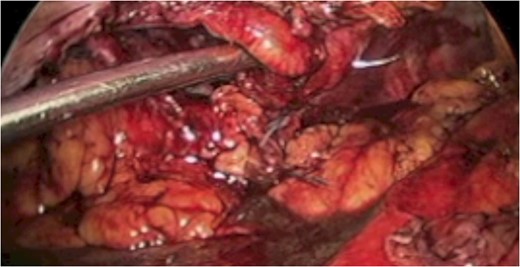
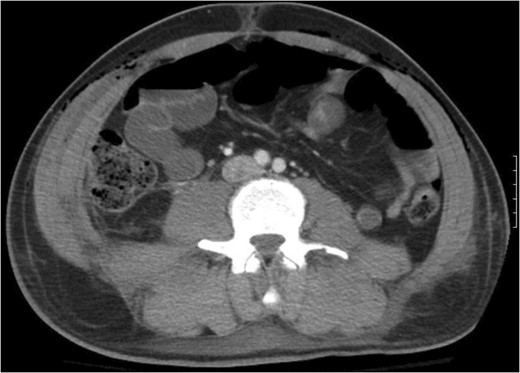
A 43-year-old male patient presented with a right-sided traumatic lumbar hernia after a blunt mechanism. The patient had been pinned between a dirt-mover’s claw arm resulting in a crush mechanism. He sustained injuries to the lumbar spine, sacrum, abdominal wall and 12th rib. On presentation, he did not have clinical or radiographic evidence necessitating abdominal exploration and was observed in a monitored setting. Computed tomography imaging demonstrated a Grynfeltt defect with herniation of the ascending colon and cecum through an area defined by the 12th rib, quadratus lumborum and internal oblique (Figures 1 and 2). After several days of observation and recuperation, the patient continued to have significant pain overlying the hernia site. We electively brought him to the operating room on post-injury Day 4. A laparoscopic repair of the traumatic hernia was performed. Key operative steps included: (i) Wide exposure of the hernia defect via incision of the peritoneum and transversalis as well as mobilization of the ascending colon and duodenal sweep (Figures 3 and 4). (ii) Primary repair of the defect with intra-corporeal suturing of the oblique musculature (Figures 5 and 6). (iii) Placement of an underlay mesh with appropriate redundancy at least 4 cm in all directions around the defect and seating against the iliac crest (Figure 7). Post-operative imaging demonstrates obliteration of the hernia defect and restoration of the abdominal wall (Figures 8 and 9). The patient has recovered, returned to the work force and has no pain or bulge at the repair site 6 months after injury.

The traumatic lumbar hernia is seen on the right side of the abdominal wall above the iliac crest on computed tomography.
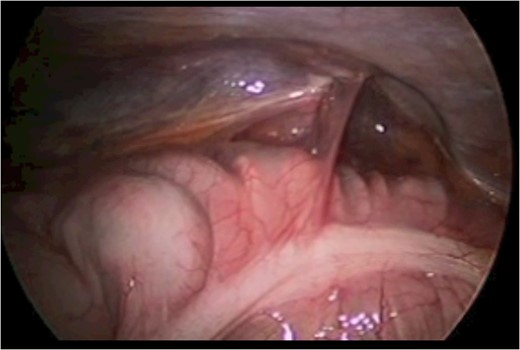
With the patient in the left lateral decubitus the herniated right colon spontaneously reduces and the hernia is demonstrated.
Step 1 begins with incision of the peritoneum overlying the hernia.
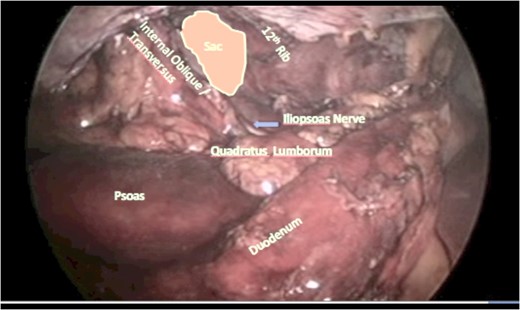
The wide mobilization completed.
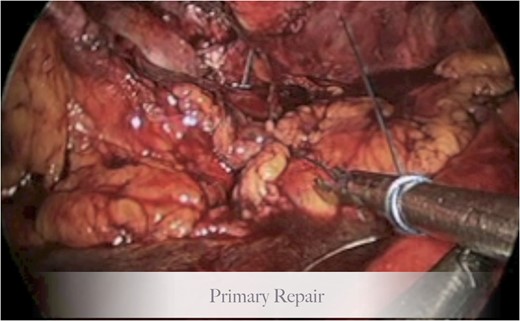
Step 2, primary repair of the hernia.
Autologous tissue is used for the primary repair.
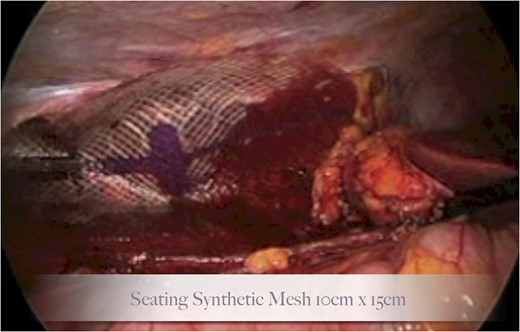
Seating of the synthetic mesh underlay.
Recreation of the abdominal wall contour is seen on the post-operative computed tomography.
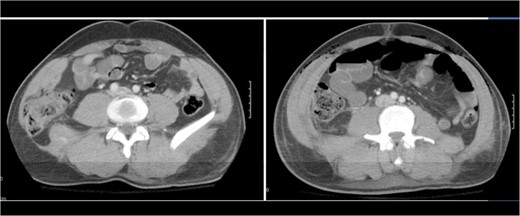
A comparison of pre-operative and post-operative imaging.
DISCUSSION
Traumatic abdominal wall hernias are a rare injuries following blunt trauma. Significant force is required and hernias are likely to occur due to abrupt deceleration at fixation points within the abdomen. One location is the lateral muscular insertion of the abdominal wall onto the iliac crest. In several studies, blunt traumatic hernias are most frequently found in the lumbar triangle above the iliac crest [3, 4]. These are injuries caused by great force, the initial management of patients centers around the identification and management of other concomitant intra-abdominal injuries. Greater than 60% patients may have other abdominal injuries [5]. Diagnosing and managing these issues precedes determining the need for hernia repair.
Having established a patient’s stability and candidacy for repair of their hernia, the next questions are when and how to operate? It has been advocated to delay repair in these patients and to use autologous tissue for the repair [6] This approach creates several challenges. It runs the risk of the hernia enlarging while awaiting repair. The patient may be in discomfort or unable to work while awaiting repair. And if a repair is performed with only autologous tissue, there may be substantial risk of recurrence. Advances in minimally invasive surgery have brought new options to the management of this challenging problem.
Delayed repairs of traumatic abdominal wall hernias using tension free techniques have been described and can be performed safely [7] Achieving an autologous tissue, tension free repair with fixation to the iliac crest can be hard. Adding synthetic mesh coverage unless contraindicated by contamination is useful [8] To these concepts, we would add through the presentation of our case study that this can be performed safely both early after an injury and via a laparoscopic approach. It is our feeling that this will result in the effective management of the hernia while also improving patient comfort and shortening time of disability. Clearly, this is an area that could benefit from further study and we would lend our voice to that of other authors suggesting that a larger prospective study with an appropriate follow-up period is the best way to generate reliable treatment algorithms [9] These types of studies should include early laparoscopic repair, as we believe it is feasible and safe.
ACKNOWLEDGEMENT
None.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}