





Abstract
Spillage of gallstones (6–40%) are common during laparoscopic cholecystectomy. Development of intraperitoneal and perihepatic abscesses are relatively rare (<0.1%). However, it may pose a diagnostic dilemma mimicking intra-abdominal tumor due to their similar radiologic appearance. Case Report: We present a 57-year-old woman with history of cholecystectomy 8 years prior who presented with a suspected diagnosis of incarcerated port site hernia with associated radiological evidence of an intra-abdominal tumor. The histological examination of the resected tumor revealed a chronic abscess. It reminds us the importance of careful removal of the stones especially in the setting of acute cholecystitis and should prompt the treating physician about this late possible complication.
INTRODUCTION
Laparoscopic cholecystectomy is the goldstandard treatment of symptomatic cholecystolithiasis and is performed in most of the surgical units. However, gallbladder leakage is a frequently occurring incident ranging from 6 to 40% [1, 2]. The dropped gallstones during this procedure can lead to the formation of an intra-abdominal abscess, which may pose a diagnostic dilemma mimicking intra-abdominal tumors or parasitic infections due to their similar radiologic appearance.
CASE REPORT
A 57-year-old woman was admitted to our institute (Spital Visp, Spitalzentrum Oberwallis) on 16 February 2017 with a suspected diagnosis of incarcerated port-site hernia following laparoscopic cholecystectomy 8 years ago. The port site hernia appeared 4 years ago and it was reducible without any obstructive symptoms. The patient initially consulted her general practitioner due to progressive pain and irreducible swelling at the site of the pre-existing hernia and was referred to us for further treatment. A CT scan revealed bowel contents and omentum in the hernial sac with an incidental finding of an around 6.5 cm in diameter mesenterial tumor in the jejunal area (Fig. 1).
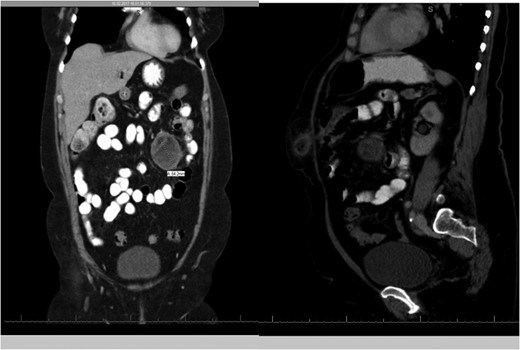
CT scans of the abdomen showing the mass.
The patients medical history reports past treatment with chemotherapy and radiotherapy for Hodgkin's lymphoma ~15 years ago and laparoscopic cholecystectomy followed by an ERCP and endoscopic papillotomy 8 years ago due to symptomatic cholecystolithiasis. Apart from a positive history of cancer in the family she presented with no B symptoms.
An emergency laparotomy with tumor and small bowel segment resection (Fig. 2) and primary side to side anastomosis with closure of the hernial defect after reduction of the contents were carried out. The histological examination of the resected mass revealed a encapsulated fibrosing process with foam cells and foreign body giant cells which was interpreted as a chronic well fibrosed abszess (Fig. 3). Immunohistolochemical evaluation revealed a mixed population of T and B lymphocytes. It showed strong staining of the cells for CD 20, CD 79a, CD 3 and CD 5 with no coexpression of CD 10 and BCL 1. The staining of markers CD 15 and CD 30 for Hodgkin lymphoma were negative.

Macroscopic view of the resected tumor.
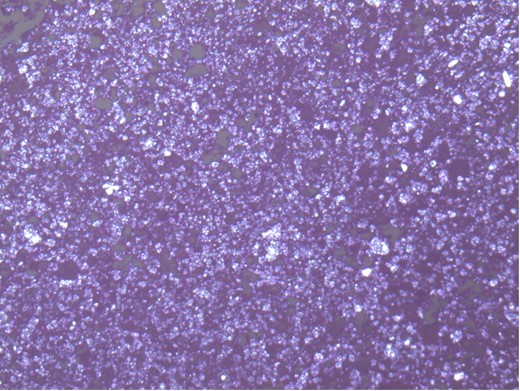
Microscopic appearance of chronic abscessing inflammation with large areas of pink necrotic tissue that are bordered by granulation tissue with numerous prominent capillaries filled with blood, foam cells and foreign body giant cells.
The postoperative evolution was uneventful and the patient was released on eighth postoperative day with a clean wound.
DISCUSSION
Complications following spilled or lost stones following open cholecystectomy have been rarely described. Infact, bile leak and spilled gallstones are often asymptomatic in 90% of the cases apart from presenting with incidental findings on postoperative CT scans carried out for other reasons. Spilled stones was initially reported as a benign complication of laparoscopic cholecystectomy with no consequences [1, 3]. Zehetner et al. reported that in 8.5% of patients following lost gallstones can lead to complications. The risk factors for developing complications were acute cholecystitis with infected bile, pigment stones, multiple stones (>15), increased age, stone size (>1.5 cm). Careful removal of as many spilled stones, intense irrigation and suction, use of intra-abdominal bags and laparoscopic graspers have been recommended. To avoid recurrence interventional abscess puncture without stone removal is not recommended by the same author [4].
Informed patient consent about this late complication could help avoid misunderstanding and develop better surgeon–patient trust.
CONCLUSION
Spilled stones left inside the peritoneal cavity after laparoscopic cholecystectomy could lead to complications, in our case an abszess mimicking an intra-abdominal tumor. It reminds the surgical community of the importance of careful removal of the stones especially in the setting of acute cholecystitis. Abscesses as well as tumor like intra-abdominal lesions in unusual sites following laparoscopic cholecystectomy should prompt the treating physician about this late possible complication.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}