





Abstract
Venous aneurysms often present as painful masses. They can present either in the deep or superficial venous system. Deep venous system aneurysms have a greater risk of thromboembolism. Though rare, there have been case reports of superficial aneurysms and thrombus causing significant morbidity such as pulmonary embolism. We present a case of an anomalous greater saphenous vein connection with an aneurysm and thrombus resulting in a pulmonary embolism. This is the only reported case of an anomalous greater saphenous vein connection with aneurysm and thrombus, which eventually led to a pulmonary embolism. Recognition of the morbidity and mortality associated with superficial venous aneurysms can help prevent catastrophic outcomes such as pulmonary embolism. Surgical intervention on large symptomatic superficial venous aneurysms may be the optimal treatment in preventing unwanted complications compared to anticoagulation alone.
INTRODUCTION
Venous aneurysms often present as painful masses. They can present either in the deep or superficial venous system. Deep venous system aneurysms have a greater risk of thromboembolism [1]. Though rare, there have been case reports of superficial aneurysms and thrombus causing significant morbidity such as pulmonary embolism [2]. We present a case of an anomalous greater saphenous to greater saphenous vein connection with an aneurysm and subsequent thrombus resulting in a pulmonary embolism.
CASE REPORT
A 57-year-old Nepali female presented to the emergency department with right lower quadrant abdominal pain and associated mass. She never had any previous episodes of pain and denied trauma to the area. The mass was first noted 2 years before presentation. It was initially the size of a pea, and had grown in size over the last 2 years. On exam, the patient had an erythematous non-pulsatile, 2 × 3 cm2 mass that was non-tender to palpation. The mass had a positive doppler signal, and the patient had palpable dorsalis pedis and posterior tibial pulses bilaterally.
On CT and ultrasound imaging of the abdomen, the patient was found to have an anomalous venous connection between the left and right saphenous veins. The connection traversed across the anterior abdominal wall and contained an aneurysmal segment close to the right saphenofemoral junction that was 3.6 cm in diameter and was partially thrombosed (Figs 1 and 2). The patient had a duplex ultrasound on hospital day one that showed the femoral veins to be patent bilaterally. Systemic anticoagulation was started with warfarin. On hospital Day 2, the patient’s pain improved and she was subsequently discharged on warfarin therapy before her INR was therapeutic with an outpatient lower extremity venous duplex to ensure no further progagation of the thrombus.
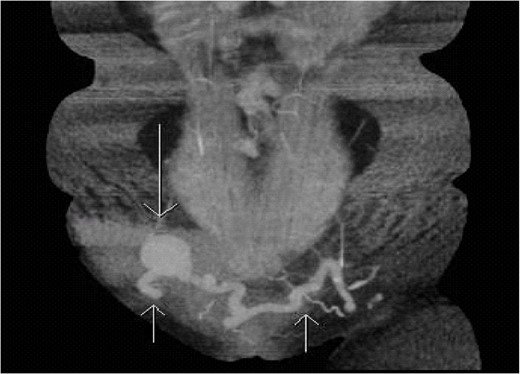
Coronal section of CTA of the abdomen/pelvis capturing the anomalous connection between the left and right greater saphenous veins with an aneurysm near the right saphenofemoral junction. Short arrows pointing up shows the tortuous connection of the greater saphenous veins. Long arrow pointing down demonstrates an aneurysm in the anomalous saphenous vein connection.
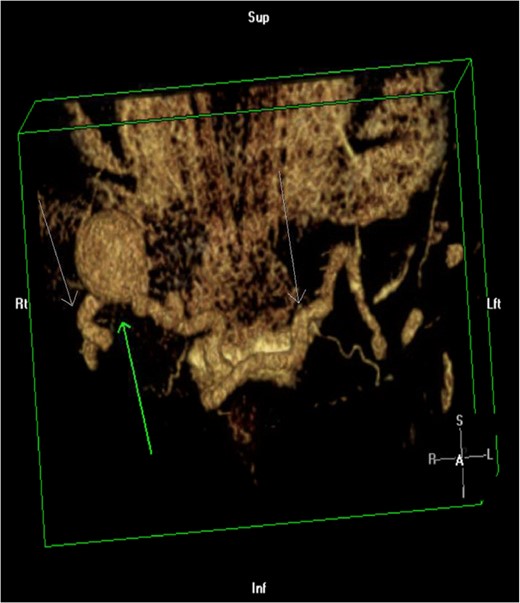
3D reconstruction of CTA of the abdomen/pelvis. Green arrow pointing up demonstrates an aneurysm in the anomalous saphenous vein connection. White arrows pointing down shows the tortuous connection of the greater saphenous veins.
Four days after her initial presentation, her venous duplex showed acute deep venous thrombosis in the left common femoral vein with more subacute thrombus in the left popliteal vein, the left greater saphenous vein and the left lesser saphenous vein. The patient was referred to the emergency department from the outpatient imaging facility and her INR was found to be 1.7. She was given therapeutic subcutaneous enoxaparin injections and discharged with instructions for her continued outpatient warfarin therapy.
The patient then presented to the emergency department on the sixth day after initial presentation with chest pain and dyspnea. Her INR was now 2.3. On CT imaging of the chest, it was discovered that the patient had a pulmonary embolus in a right lower lobe posterior segmental arterial branch. She was subsequently admitted and placed on therapeutic heparin. Her symptoms quickly resolved and she was discharged on warfarin therapy with a therapeutic INR.
DISCUSSION
Our case is the only known reported case of an aneurysm in an anomalous venous connection between the left and right saphenous veins. Historically, surgical management of venous aneurysms of the extremities was reserved for deep venous aneurysms because of their high risk of thromboembolic complications despite anticoagulation whereas superficial extremity aneurysms are rarely symptomatic and at low risk of rupture, therefore the only indications for surgery were for disfiguring lesions [3]. Aneurysms of the saphenous venous system are classified into four types. Type 1 are located in the proximal third of the saphenous vein, and are the most common with an average diameter of ~1.5 cm. Type 2 are located in the shaft of the saphenous vein in the distal third of the leg. Type 3 are types 1 and 2 in the same lower extremity. Type 4 are superficial short saphenous vein aneurysms [4]. These saphenous vein aneurysms have associated morbidity because there have been case reports of types 1 and 2 saphenous vein aneurysms which have resulted in pulmonary embolism [2].
This patient would have warranted aneurysmal ligation based on size criteria alone, however, the patient had left iliac vein atresia and her anomalous connection was serving as her main venous outflow for her leg. Iliac vein compression syndrome (May–Thurner syndrome) may have been responsible for her left iliac vein atresia and subsequent reconstitution of flow through this saphenous vein connection (Fig. 3). There has been only one other reported case of May–Thurner syndrome where there was reconstitution of flow through an anomalous connection (left femoral to right greater saphenous vein connection), but no mention of an aneurysm within the anomalous connection [5]. Reports in the literature also suggest that there may be a decreased recurrence of ileofemoral vein thrombosis in May–Thurner syndrome patients who undergo left iliac vein stenting combined with anticoagulation [6].

CTA of Abdomen/pelvis showing left iliac vein atresia. Short arrow is pointing to the inferior vena cava and long arrow is pointing to the right iliac vein. The left iliac vein is absent.
In future cases, we recommend early ligation of the aneurysmal saphenous vein connection anomalies to prevent the catastrophic outcome of pulmonary embolism. Venography can be considered if there is concern that ligation would result in obliteration of the main venous outflow in May–Thurner syndrome patients. If venography demonstrates that the anomaly is the main venous outflow then a venous bypass procedure or stenting of the iliac vein to reestablish venous outflow should be considered before ligation of the saphenous vein anomaly aneurysm.
Conflict of Interest statement
None declared.

{kind=link}
{kind=link}
{kind=link}