





Abstract
We present the case of a 64-year-old man who was referred to our service after sustaining a self-inflicted nail-gun injury to his chest. He received three nails penetrated into his chest. Computer tomography revealed no massive haemorrhage or damage to major vessels. He underwent an emergency sternotomy, two nails caused pericardial perforation and myocardial injury were noted easily and removed easily via sternotomy. Myocardial injury showed a trajectory near the junction of the left anterior descending artery and the diagonal artery with no significant bleeding appreciated. The third nail was deep in the lung parenchyma at the hilum. A pacemaker magnet was used to locate the third nail, which was subsequently removed. Our case demonstrates the use of magnets in emergency surgery, to locate and remove metallic foreign bodies.
INTRODUCTION
Penetrating thoracic injury caused by a nail gun is life threatening and requires urgent management following ATLS protocol, and in most cases surgical intervention. Imaging can be employed in case of a stable patient, such as in our case.
Nail gun related penetrating injuries are well documented in the extremities. There is handful of cases reported in thoracic nail gun injury. Locating and retrieving metal foreign bodies can be challenging during an emergency operation. In recent years, the incidence of self-inflicted cases has been on the rise [1, 2].
The main strategy in targeting such cases nowadays is that of a standard visual search followed by the use of intra-operative imaging when required. We report a case of a 64-year-old man with three metal nails in his chest where a pacemaker magnet was used intra-operatively to help locate and remove one of the nails.
CASE REPORT
A 64-year-old man referred to our institution with self-inflicted penetrating chest injuries with an electric nail gun. This was in response to express his frustration towards an expensive non-functioning product purchase. Patient used an electric driller to fire in three nails on the chest between left anterior axillary line and left lateral sternal border. Upon arrival to emergency department, on initial assessment according to ATLS protocol, his Glasgow coma score (GCS) was 15, hemodynamically stable with three puncture wounds in his chest medial to his left nipple. He also sustained full thickness electrical burns on the left middle and index fingers and fractured right middle, ring and little fingers. Chest radiograph showed three nails of close proximity to the heart, and a left sided pneumohaemothorax. A chest drain was inserted and a CT thorax was performed (Figs 1 and 2).
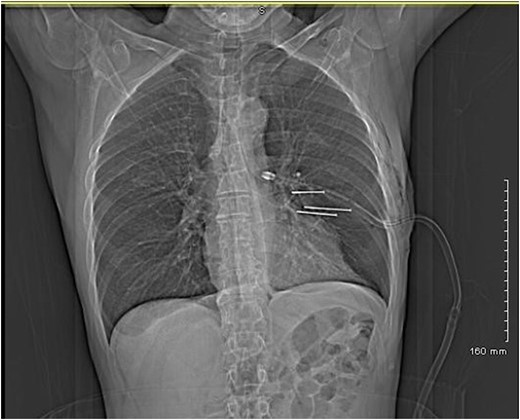
CT thorax showing the three nails on coronal view.
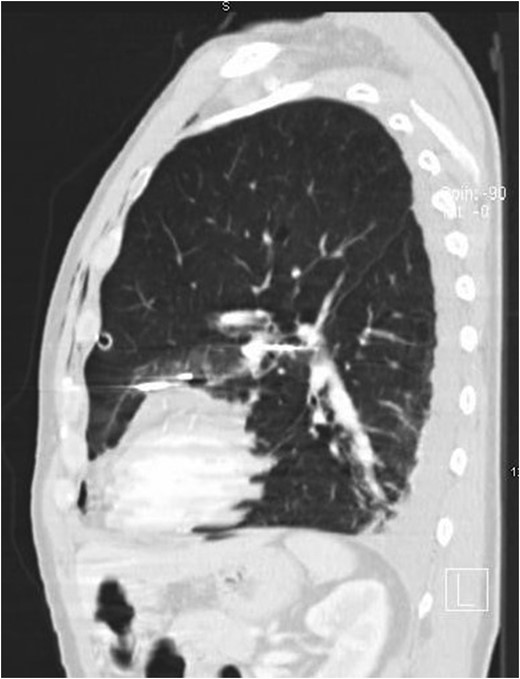
CT thorax showing the three nails on sagittal view.
Past medical and surgical history included hypertension, asthma, diverticulosis and a right mastoidectomy. He has a smoking history of 25 pack years and a history of alcohol abuse though reports to have been abstaining for the last 20 years. He has no previous history of psychiatric illness or contact with mental health services.
The patient underwent a sternotomy for removal of the three nails. Two nails were easily visible and removed. They caused pericardial perforation and myocardial injury. The third nail was difficult to locate. Myocardial injury showed a trajectory near the junction of the left anterior descending artery and the diagonal artery with no bleeding appreciated. A magnet was then used to locate the third nail which was found to be deep in the hilum of the lung. The magnet was then used to gently ‘milk’ the nail into a more superficial position. Once the nail was more easily accessible, it was removed.
The patient recovered well post-operatively and he was discharged to psychiatric care.
DISCUSSION
A case of a lost metal during surgery whether that of foreign bodies as in our case or of lost needles can be quite challenging to even the most experienced surgeons. Currently, the protocol involves a combination of standard visual search and intra-operative imaging [3]. This approach can lengthen operative time, cause iatrogenic injury during a rigorous search, and increase operative costs [4].
There was minimal literature available around the use of magnets in thoracic surgery. What the literature did reveal was the use of magnets in laparoscopic and maxillofacial surgery in cases of lost retained needles. Chittenden et al. [1] reported the use of an electromagnet to retrieve a broken fascia needle during frontalis sling surgery. In laparoscopic surgery, Barto et al. [2] concluded that the use of a laparoscopic magnet was the safest and most efficient way of retrieving lost needles intra-operatively. Moreover, Padilla et al. [5] found that the use of magnet graspers in laparoscopic surgery improves triangulation and ergonomics while reducing the number and size of abdominal incisions.
Conflict of Interest Statement
The authors declare that they have no competing interests.
Learning points
Locating and removing lost metal can be challenging to even the most experienced surgeons.
Use of magnets intra-operatively is an option that could be considered in situations where it is tough to locate or remove metal foreign bodies.
The use of magnets intra-operatively reduces the risk of iatrogenic injury, length of operation and cost.
Consent
Written informed consent was obtained from the patient for publication of this Case report and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal.

{kind=link}
{kind=link}