





Abstract
Acute Type A aortic dissection is a surgical emergency. Urgent repair is indicated to avoid complications such as acute aortic insufficiency, coronary ischemia and aortic rupture with cardiac tamponade. This report details the management of a patient with acute Type A aortic dissection complicated by an extensive anterolateral myocardial infarction and cardiogenic shock who was successfully bridged to transplantation with a total artificial heart.
INTRODUCTION
Acute Type A aortic dissection is a surgical emergency. Urgent repair is indicated to avoid complications such as acute aortic insufficiency, coronary ischemia and aortic rupture with cardiac tamponade. Aortic dissection associated with myocardial infarction is an extremely rare condition and is associated with poor outcomes especially with treatment delay [1–3].
This report details the management of a patient with acute Type A aortic dissection involving the left main (LM) coronary artery complicated by an extensive myocardial infarction and cardiogenic shock who was successfully bridged to transplantation with a total artificial heart.
CASE REPORT
Case presentation
The patient is a 53-year-old man with a history of hypertension. He sustained an out of hospital cardiac arrest secondary to an anterolateral ST elevation myocardial infarction (STEMI). He was loaded with Prasugrel and heparin and was treated with drug eluting stents in the LM, proximal left anterior descending (LAD) and left circumflex coronary arteries. Because of persistent cardiogenic shock, an intra-aortic balloon pump was placed. Transthoracic echocardiogram (TTE) revealed severe left ventricular (LV) dysfunction with an ejection fraction of 25%, moderately severe aortic regurgitation, aortic root dissection and he was subsequently transferred to our institution. Upon arrival, he was mechanically ventilated and required increasing doses of inotropes. He experienced frequent supraventricular and ventricular arrhythmias. CT scan of the thoracic aorta revealed a dilated aortic root (maximum transverse diameter of 5 cm) and a dissection flap involving the non-coronary and left coronary sinuses with concern of transmural hypoperfusion of LAD territory (Fig. 1).
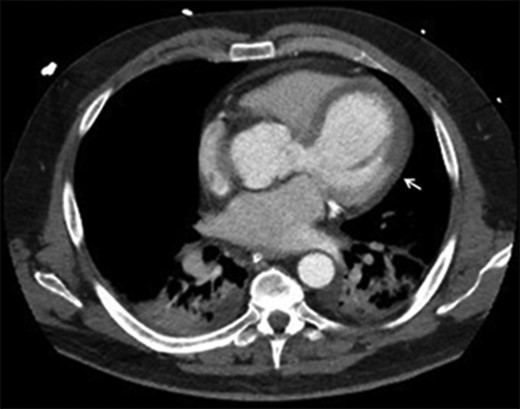
CT aorta: arrow points at the differential myocardial enhancement corresponding to large area of infarct.
With the persistent hemodynamic instability, he suffered acute kidney and hepatic injury. Veno-arterial extracorporeal membrane oxygenator (ECMO) was inserted with restoration of satisfactory tissue perfusion.
The patient was presented to our heart transplant committee and was found to be a suitable candidate for implantation of total artificial heart (TAH) as a bridge to transplantation.
Operation
Upon pericardial entry; hematoma and ecchymosis involving the anterior aspect of both the aorta and pulmonary artery was noted (Fig. 2) and this extended to the majority of the LV surface. Cardiopulmonary bypass was established with weaning off ECMO. As the tear was limited to the aortic root, the ascending aorta was cross clamped and aortotomy performed. A complex tear was noted, mainly in the left coronary sinus of Valsalva (Fig. 3) and extending around the LM coronary ostia and which we believe was the cause of his STEMI. Cardiectomy was performed. Once deep hypothermia was achieved, systemic circulatory arrest was performed and a Dacron graft was used to replace the ascending aorta and the undersurface of the aortic arch. Systemic perfusion was resumed and attention was redirected toward implantation of TAH (Syncardia systems, Inc). Prolene sutures were used in a running fashion to sew the remnants of the mitral and tricuspid valves to the ventricular muscle. These were then sutured to the quick-connect cusps (Fig. 4). The pulmonary and aortic cuffs were sutured to the pulmonary artery and ascending aorta grafts respectively. The drivelines were tunneled and connected to the device console. The patient was transitioned from cardiopulmonary bypass to the total artificial heart (Fig. 5). After satisfactory hemostasis, the chest was closed and the patient was transferred to the ICU on minimal inotropic support. He was transferred to the regular nursing unit 2 weeks after TAH implantation. He successfully underwent cardiac transplantation after 173 days of uncomplicated support.
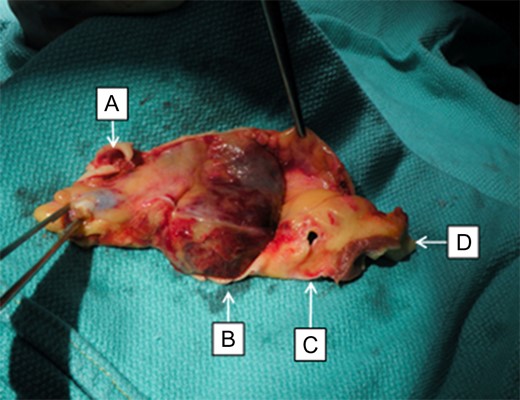
(A) Left main coronary artery with a tear and coronary stent in place. (B) Hematoma involving the aortic root at the non-coronary sinus. (C) Right coronary artery ostium. (D) Septal muscle.
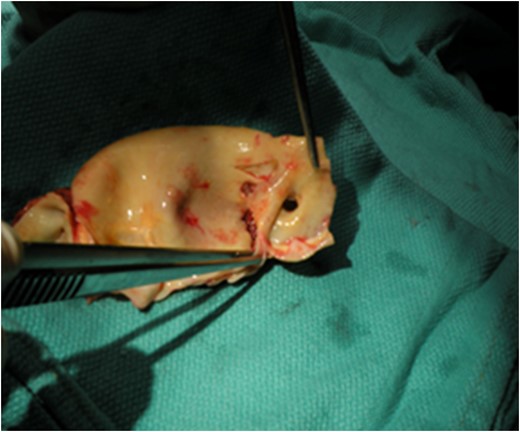
Intimal flap involving left coronary sinus and left main coronary ostium.
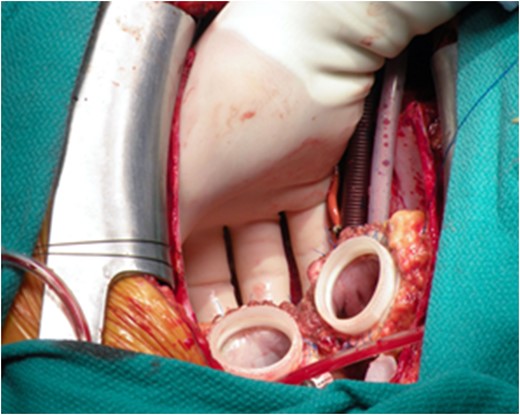
The quick-connect cusps were sutured to the annulus of both mitral and tricuspid valve.
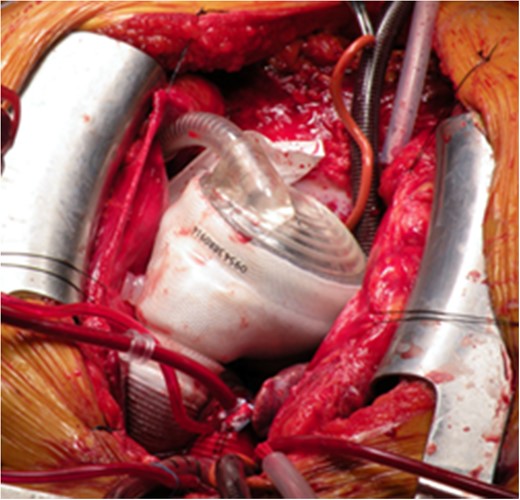
Implantation of TAH was completed.
Pathological examination
The explanted heart showed an extensive transmural myocardial infarction involving the antrolateral wall, entire basal septum and whole LV apex.
DISCUSSION
Previous studies showed that aortic dissection is associated with increased operative mortality when myocardial ischemia, hemodynamic instability or renal failure are present [4]. The International Registry of Acute Aortic Dissection (IRAD) reported hemodynamic instability and shock as independent predictors of mortality [5]. All of these risk factors coexisted in this patient.
In this patient, because of the aortic root dissection and aortic valve regurgitation, a complex aortic root replacement with implantation of a dissected coronary ostium would have been required along with multi-vessel grafting. This technically challenging procedure was being considered in a patient who appeared to have suffered a large if not fatal anteroseptal myocardial infarction. Because of these factors a total artificial heart as a bridge to transplant was chosen as the ideal procedure.
This is the first reported case of TAH support for aortic root dissection in cardiogenic shock. The outflow conduit of the TAH uniquely addressed the problems presented by this case. There was no need to reimplant the dissected LM coronary artery, a mechanical valve treated the aortic regurgitation and the dilated ascending aorta was replaced.
CONCLUSION
In the setting of mechanical complications after a large myocardial infarction—large inferior ventricular septal defect with right ventricular failure, papillary muscle disruption and LV failure, myocardial rupture and large myocardial infarction or chronic heart failure in the presence of multiple prosthetic valves, the total artificial heart is an ideal method of mechanical support. It addresses both pump function and structural abnormalities which are much more challenging to manage by conventional repair and use of circulatory support with a LV assist device.
CONFLICT OF INTEREST STATEMENT
The authors have no relationship with industry to disclose.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}