





Abstract
Cases of skeletal muscle metastasis of esophageal carcinoma are very rare, with few reports of long-term survival. We report a case of long-term survival after surgical resection of skeletal muscle metastasis. A 56-year-old man with advanced esophageal cancer and early gastric cancer underwent thoracoscopic esophagectomy, 2-field lymph node dissection, partial gastrectomy and gastric tube reconstruction. Six months later, cervical lymph node metastasis and mediastinal lymph node recurrence were found. Therefore, the patient underwent cervical lymph node dissection and adjuvant chemoradiotherapy. Two years and 3 months after the esophagectomy, a muscle metastasis was found in the left shoulder, and he underwent tumor dissection, followed by adjuvant chemotherapy for a year. There has been no sign of recurrence since, even 13 years after the esophagectomy. We believe our aggressive surgical treatment might have led to long-term survival.
INTRODUCTION
Esophageal cancer is an aggressive disease that frequently metastasizes to the lungs, pleura, liver, stomach, peritoneum, kidney, adrenal gland and bone, but metastasis to skeletal muscles has been infrequently reported in the literature in a few small series and clinical reports [1–7]. Despite recent improvement in surgical techniques and adjuvant therapies, mortality rate is very high once metastasis occurs, and few patients with skeletal muscle metastasis of esophageal cancer survive long-term.
We report the case of a patient who survived long after the surgical resection of skeletal muscle metastasis after esophagectomy for squamous cell carcinoma (SCC) of the esophagus.
CASE REPORT
A 56-year-old man presented to our institution with esophageal and gastric cancer. Esophagogastroduodenoscopy (EGD) demonstrated a type 2 tumor occupying one-third of the circumference of the esophagus and measuring 28–33 cm from the incisors (Fig. 1). Endoscopy revealed that the tumor invaded the muscularis propria and biopsy revealed SCC. Moreover, a type 0-IIb tumor was located at the lesser curvature of the angle of the stomach. Endoscopy revealed invasion of the mucosa and biopsy revealed adenocarcinoma (Fig. 2). Computed tomography (CT) showed no enlarged lymph nodes in the mediastinum or distant metastasis in the liver or lung. Therefore, the patient underwent thoracoscopic esophagectomy (video-assisted thoracic surgery for esophagus), 2-field lymph node dissection, partial gastrectomy and gastric tube reconstruction via a retrosternal route for the advanced esophageal and early gastric cancers. Histopathologic analysis revealed Stage II (type 2, T3, ly2, v0, N0, PM0, DM0) esophageal and Stage I (type 0-IIb, T1, ly0, v0, N0) gastric cancer, with positive horizontal margins of dissection of the gastric cancer. Therefore, as additional treatment, we performed argon-plasma coagulation around the dissected gastric mucosa postoperatively.
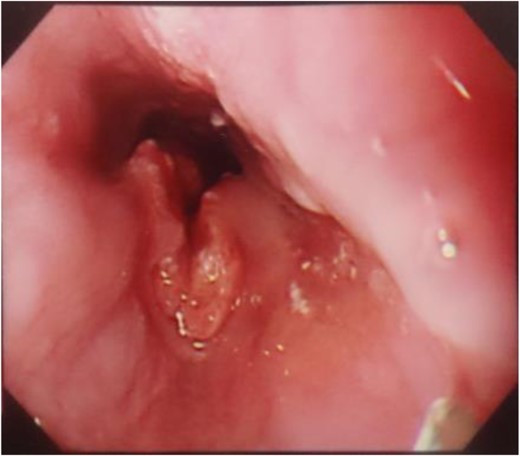
A type 2 tumor occupying one-third of the circumference of the esophagus on esophagogastroduodenoscopy.
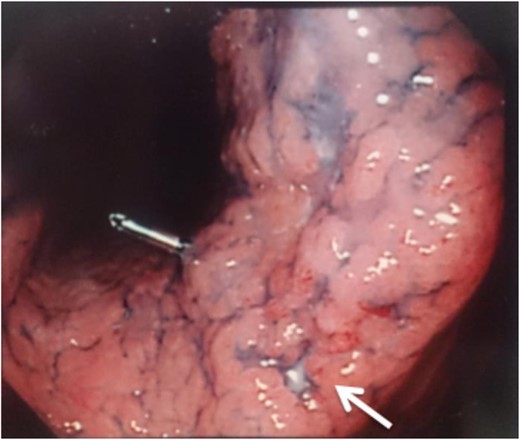
A type 0-IIb tumor located at the lesser curvature of the angle of the stomach on esophagogastroduodenoscopy.
Three months later, tumor marker levels increased, and 6 months later, CT revealed cervical lymph node recurrence and mediastinal lymph node metastasis. Therefore, the patient underwent cervical lymph node dissection. Histopathology revealed metastatic SCC and the patient received adjuvant chemoradiotherapy (nedaplatin 20 mg for 5 days, fluorouracil 500 mg for 7 days, 40 Gy). The patient was followed up.
Two years and 3 months after esophagectomy, he complained of pain in the left shoulder. A mass was found between the trapezius and supraspinatus on CT and magnetic resonance imaging (Fig. 3). 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) demonstrated increased levels of FDG accumulation in the left shoulder. Needle biopsy demonstrated class V (unclear type of carcinoma) disease. Therefore, we performed tumor dissection for muscle metastasis, and the histopathologic diagnosis was SCC. The patient thus underwent adjuvant chemotherapy with S-1 (80 mg/day) administered 4 weeks on/2 weeks off schedule for 1 year.
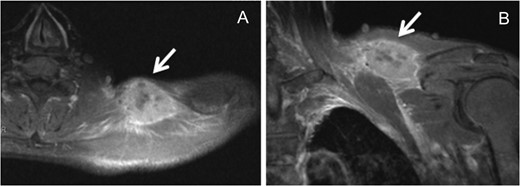
A hyperintensity mass between the trapezius and supraspinatus on T1-weighted magnetic resonance imaging (A, axial view; B, coronal view).
Five years after esophagectomy, EGD revealed red and easy-bleeding mucosa inside his gastric tube, and biopsy showed Group V (well-differentiated) adenocarcinoma. The depth of invasion was thought to be deeper than the submucosa by EGD, so we performed total dissection of the gastric tube and right colon reconstruction via the retrosternal route. Histopathology demonstrated Stage Ib disease (well-differentiated tubular adenocarcinoma, Type 3, T2, ly0, v0, N0). We found no association between the first gastric tumor and this tumor. Patient condition remained good, and there was no sign of recurrence 13 years after esophagectomy.
DISCUSSION
Skeletal muscle metastasis of carcinoma is rare. The most common primary lesion is carcinoma of the lung and the most common locations for metastasis are the skeletal muscles of the lower limb [8]. The skeletal muscles of the thigh and calf were the most common anatomical sites, whereas the skeletal muscles of the upper limb and other sites were less involved. In 75% of patients, the skeletal muscle metastasis presented as a ‘painful mass’, which might have occurred more often in patients with skeletal muscle metastasis than in those with soft tissue sarcomas [8]. In our case, metastasis also occurred in the shoulder, accompanied by pain.
According to Shoda et al. [7], a soft tissue mass caused by metastatic carcinoma is easily misdiagnosed as soft tissue sarcoma on physical examination and imaging studies. FDG–PET is more accurate than CT, especially in body regions that are not routinely evaluated by CT [7]. In our case, FDG–PET was useful to detect muscle metastasis.
Despite recent improvement in surgical techniques and adjuvant therapies, mortality rate after metastasis is very high. Tuoheti et al. [8] reported that 7 of 12 patients died in 2–19 months (average, 9 months) after detection of skeletal muscle metastasis; only one patient was continuously disease-free for 92 months after wide excision of the metastatic lesion. This long-surviving patient had lung carcinoma. Cincibuch et al. [9] reported five patients with esophageal carcinoma metastatic to the skeletal muscle; all five died in 2–31 months after diagnosis despite treatment. We found no long-surviving case of skeletal muscle metastasis from esophageal SCC except ours.
Cincibuch et al. [9] reported that, similar to metastases to other locations, the best control might be obtained with surgery, which, however, was meaningful only in patients with isolated skeletal muscle metastasis. External beam radiation should be reserved for patients with inoperable or recurrent skeletal muscle metastasis, including patients with metastases at other sites, and best results might be obtained when combining radiation with platinum-based chemotherapy.
In our institution, if possible, we normally perform surgery first for metastatic esophageal carcinoma. In this case, we were able to perform surgical dissection twice for the metastatic esophageal carcinoma (dissection of cervical lymph nodes and of skeletal muscle metastasis) because the metastasis was isolated. After dissection of the skeletal muscle metastasis, we performed adjuvant chemotherapy for a year because the skeletal muscle metastasis was thought to be hematogenous metastasis. There was no sign of recurrence even 13 years after esophagectomy. We suppose our aggressive surgical treatment might have led to this long-term survival. In previous reports, the prognosis of skeletal muscle metastasis of esophageal carcinoma has been very poor. However, we believe it is important not to give up and to choose aggressive surgical treatment.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}