





Abstract
Pilomatrixoma is a benign tumor of hair follicle matrix cells. The majority of all pilomatrixomas were reported to affect the head–neck region and rarely the upper extremity. We present a case of left-leg pilomatrixoma, which is a extremely rare localization, in a 10-year-old boy.
INTRODUCTION
Pilomatrixoma is a benign tumor of hair follicle matrix cells. It is also known as the calcifying epithelioma of Malherbe or trichomatrixoma. The majority of all pilomatrixomas were reported to affect the head–neck region and the upper extremities in children [1]. Pilomatrixoma appears as slow-growing solid mass in the subcutaneous tissue. Its incidence varies between 0.03 and 0.1%. This neoplasm is observed more frequently among women below 20 years of age [2]. The number of reports according to pilomatrixoma are limited in the literature. We present a case of left-leg pilomatrixoma which is a very rare localization in a 10-year-old boy.
CASE
A 10-year-old boy presented with a 3-month history of pain and swelling in the left leg. Physical examination showed a 3 × 4 cm2 solid and mobile mass along the posterior aspect of the left leg. There were no history of trauma, weight loss or previous inflammatory disease. Radiographs showed calcification on the posterolateral side of the left cruris (Fig. 1). MRI indicated a solid soft tissue mass in the posterolateral side of the left cruris, which was observed to be hypointense in the T1A series, and hyperintense in the T2A series. The mass had regular margins, and exhibited peripheral contrast enhancement with a 41 × 30 × 27 mm3 size (Fig. 2). Lipoma, epidermoid cyst, sebaceous cyst, calcified hematoma and giant-cell tumor were considered in differential diagnosis. Incisional biopsy was performed. Histopathological examination confirmed as pilomatrixoma (Fig. 3). Thus, a complete resection of the mass was performed. There has been no recurrence, either clinically or radiologically, in subsequent 1-year period.
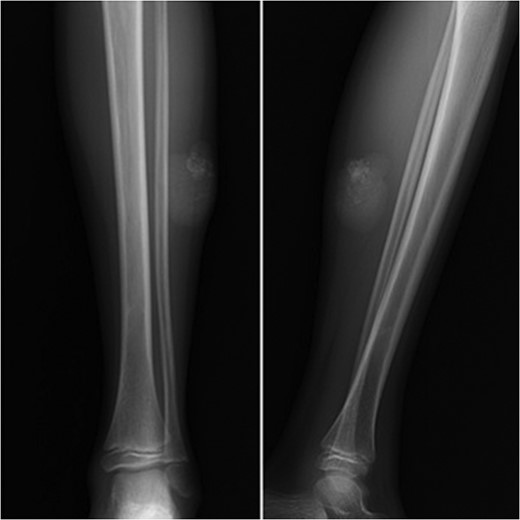
Image of calcification on the posterolateral part of the cruris.
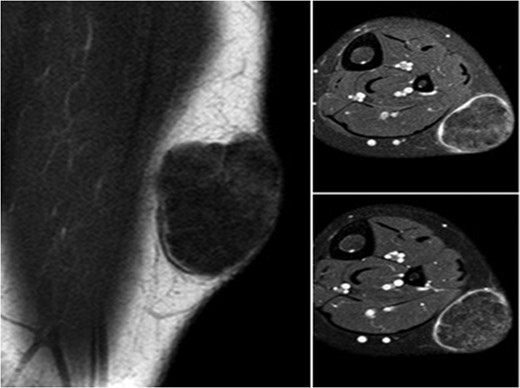
Magnetic resonance image of the homogeneous lesion, visualized with regular margins and including patch-like areas.
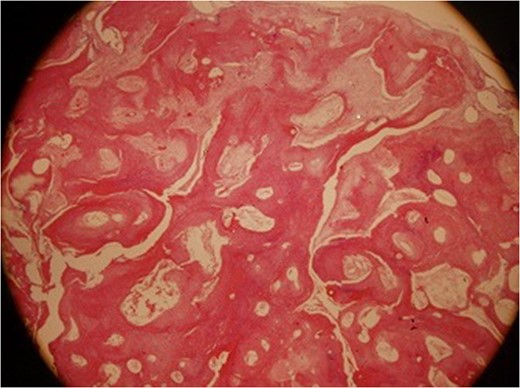
Lesion showing development in the form of irregular islands made up of a nucleate eosinophilic shadow cells, with the spindle-like fibroblastic cells between them.
DISCUSSION
Pilomatrixoma is a rare, benign epithelial neoplasm of hair follicle matrix cells. It accounts for 0.1% of all skin tumors [3]. It was first defined by Malherbe and Chenantais as a calcified tumor, and was later named as pilomatrixoma by Forbis and Helwig in 1961 [4, 5]. Although its etiology has not yet been fully elucidated, studies suggest that pilomatrixoma can develop as a result of trauma, infection, or an interruption in the hair follicle cycle [1]. Nearly 50% of all pilomatrixomas are observed in the head and neck regions as a single nodule, while multiple pilomatrixomas have been reported in 2–10% of all cases [2]. The incidence ratio between males and females is 2:3. It has been shown that the tumor is related to xeroderma pigmentosum, Gardner syndrome, Turner syndrome, sarcoidosis and Steinert disease [3, 6, 7]. Pilomatrixoma generally occurs as a single nodule consist of solid and painless subcutaneous masses between 0.5 and 3 cm with well-defined margins. It can exhibit hemangioma-like red–blue color changes on the skin because its often localized superficially [7, 8]. Malignant form that known as pilomatrixcarcinoma is capable of metastasizing to the lungs, bone, brain, skin and lymph nodes [9].
During differential diagnosis, it is necessary to consider the possibility of dermoid cyst, sebaceous cyst, calcified lymphadenopathy, ossified or calcified hematoma, foreign bodies, giant-cell tumor and lipoma [7, 8, 10]. While pilomatrixoma does not exhibit a distinct and noticeable diagnostic feature during radiological examination, the presence of calcification is an important finding (Fig. 1). Although pilomatrixoma can be preoperatively diagnosed in 40% of cases with the aid of clinical and radiological methods, definite diagnosis requires histopathological examination [10].
Standard treatment for pilomatrixoma is surgical excision. Rate of recurrence following surgery has been reported as 2–6% [10]. No recurrence was observed in our case during 1-year follow-up. The clinical characteristics of our case were in parallel with the literature. The exception that pilomatrixoma was located in the lower extremity in our case, which is an extremely rare localization, and also the tumor was 4 × 3 cm2 in size, which is close to upper size limit that usually observed in pilomatrixoma cases.
CONCLUSION
Pilomatrixoma is a rare condition whose clinical features are not well-defined. There is a high likelihood of confusing pilomatrixoma with the other types of lesions. Thus, cases have to be evaluated carefully to avoid overlooking any malignant forms, and they should also be closely monitored at frequent time intervals against to the possibility of post-operative recurrence.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}