





Abstract
The most frequent sites of distant metastasis of colorectal cancer (CRC) are primarily liver and lung, followed by brain and bone metastases. Infrequently, metastases are found in the adrenal glands. They usually have a metachronous and homolateral character. We present a case of contralateral synchronic adrenal metastasis of CRC and its surgical resolution.
INTRODUCTION
The most common sites of distant metastases of colorectal cancer (CRC) are primarily liver and lung, followed by brain and bone metastases [1]. Metastases of the adrenal glands are very infrequent and usually metachronous and ipsilateral.
We report the case of a patient with synchronous contralateral adrenal metastasis of CRC who underwent curative surgical treatment.
CASE REPORT
A 63-year-old female patient, with no medical history of relevance, presented with a palpable mass in the right flank which she first noticed a month ago, associated with chronic anemia. After performing a computed tomography (CT) scan, a circumferential thickening of the cecum and the ascending colon walls and a slight enlargement of the left adrenal gland (20 × 15 mm2 in diameter) were observed (Fig. 1). There was no evidence of liver or lung metastases. At the time of diagnosis, the serum carcinoembryonic antigen (CEA) level was 0.6 ng/ml.
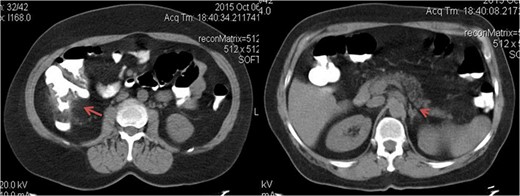
Axial tomographic view with oral contrast. The red arrow shows the tumor in the right colon and the arrowhead pointing synchronous contralateral adrenal metastasis.
Subsequently, a complete colonoscopy was performed, in which an ulcerated, stenotic and friable lesion of the cecum and ascending colon was observed and biopsied. Deferred histopathological report showed a moderately differentiated adenocarcinoma of colorectal origin.
After a complete medical assessment, a laparoscopic right colectomy was performed. The patient was discharged 3 days after de surgery without having presented complications. The final pathology report showed a low-grade adenocarcinoma with 18 negative lymph nodes; Stage II disease (pT3 pN0).
The patient remained asymptomatic during subsequent clinical check-ups. However, in the first CT scan of follow-up 3 months after surgery, a marked increase in the volume of the left adrenal gland was detected. After discussing the case at the multidisciplinary team meeting, a positron emission tomography–CT (PET–CT) scan was performed. A hypermetabolic and expansive lesion was evidenced in the left adrenal gland, of 52 × 32 mm2 in diameter, with a standardized uptake value (SUV) of 13.4, which was interpreted as an adrenal metastasis (Fig. 2). A laparoscopic left adrenalectomy was performed and the patient was discharged 48 h after an uneventful postoperative course. Pathology report was consistent with adrenal metastatic disease from a moderately differentiated adenocarcinoma of colorectal origin (Fig. 3).

PET–CT frontal view. Increased uptake and metabolism (SUV 13.1) to left adrenal level is observed.
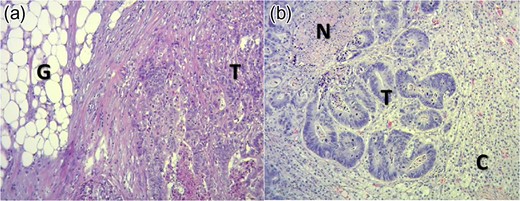
(a) Histological section of right colon with hematoxylin and eosin technique in ×400 field. It states: Tumor (T) and pericolonic fat (G). (b) Histological section of left adrenal gland with hematoxylin and eosin technique in ×400 field. Upper left to lower right are indicated: necrosis (N), tumor (T) and adrenal cortex (C).
Subsequently, the patient underwent four cycles of adjuvant chemotherapy with capecitabine and oxaliplatin, and after 10 months of follow-up there was no evidence of local or systemic disease.
DISCUSSION
The prevalence of a primary adrenal tumor found on a CT scan of patients being staged or followed-up for a known adrenal tumor, ranges from 0.35 to 5%. In turn, the prevalence of metastatic disease of the adrenal glands ranges from 38 to 57% [2]. It stands out, that these lesions should not be called incidentalomas, since they are found in the context of an oncological disease [3].
Primary tumors with the highest prevalence of adrenal metastases are breast, lung and kidney carcinomas. The incidence of adrenal metastatic lesions from CRC varies from 0.15 to 17.4% according to the literature [4]. Generally, preoperative diagnosis is difficult because adrenal metastatic lesions are not only asymptomatic but also morphologically resemble the characteristics of adrenal adenomas. That is why CRC metastases are often diagnosed at autopsy [5]. In conducting a literature review, adrenal metastases from CRC are predominantly ipsilateral and metachronous, or at least the diagnosis of the adrenal lesion was made after the initial surgical resection of the primary tumor. To the best of our knowledge, seven cases of synchronic and contralateral adrenal metastases of CRC have been reported [6].
Since metastatic adrenal lesions are usually nonfunctional and have few to no symptoms of local invasion, imaging studies are an important tool in the differential diagnosis. Tomographic features of malignant lesions include: size >3 cm, attenuation >10 Hounsfield units, heterogeneity and increased vascularity [7]. Note that the nodule found in the first CT scan of our case, lacked of all the mentioned features. Furthermore, the PET–CT findings are considered positive if the SUV in the adrenal tumor is greater than or equal to the liver. Recently it has been suggested that an SUV of 3.1 is useful in differentiating malignant and benign lesions [8]. In our case, after the resection of the primary tumor, the adrenal lesion showed a SUV of 13.4, reinforcing the oncological origin of this tumor.
Regarding the CEA level, it may contribute to the suspicion of disseminated disease or recurrence. However, as in the present case (basal CEA: 0.6 ng/ml), there are circumstances in which CEA level does not reflect the presence of systemic disease, especially when blood value is initially normal [9].
Adrenal metastases from CRC are usually a manifestation of systemic spread of the disease and as such, represent a worse medium and long-term prognosis [10]. A recent systematic review reported an average overall survival at 2 years after adrenalectomy for solitary metastatic disease of 46%. In a more recent publication, the mean time of survival ranging from 7 to 48 months, with a 5-year survival of 20–45%. Also, the surgical treatment of isolated adrenal metastasis is associated with improved quality of life. As a limitation to this analysis, it is important to note that these studies include a wide variety of primary malignancies, among which CRC represents a minority.
In conclusion the diagnosis of metastatic lesions in adrenal glands is done primarily through its incidental finding in the follow-up studies of a known oncologic disease as a result of improved and increased use of diagnostic imaging methods. Synchronous contralateral solitary metastasis of CRC is rare, but the possibility of resection improves prognosis in the short and medium term.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING
None.
CONSENT
Consent was obtained from the patient for publication.
ETHICAL APPROVAL
Ethical approval and informed consent were obtained and available upon request.
AVAILABILITY OF DATA AND MATERIALS
Data are available from the medical record of Hospital Italiano de Buenos Aires, Capital Federal, Argentina. The data cannot be publicly available due to local legal restrictions.

{kind=link}
{kind=link}
{kind=link}