





Abstract
Midline neck lumps are commonly recognized in clinical practice. Nonetheless, we present an unusual case of a 24-year-old Bangladeshi man who has a slowly growing midline neck lump. The characteristic lump did not move on swallowing and was more pronounced on coughing suggesting an external laryngocoele as a main differential. The patient underwent urgent surgical excision of the lump. Further histopathology findings were consistent with the diagnosis of a bronchogenic cyst which is deemed rare with such presentation.
INTRODUCTION
Bronchogenic cysts are rare congenital malformations arising from the tracheobronchial tree that rarely present outside the thorax. The unusual sign of lump expansion with increased intrathoracic pressure (Valsalva manoeuvre) was indicative of an airway communication, though this was not evident on imaging (Computed tomography, CT).
The pathophysiology of bronchogenic cysts illustrated the diagnostic difficulties encountered with rare lesions and highlighted the awareness of the different anatomical presentations.
CASE REPORT
A 24-year-old unemployed man of Bangladeshi origin presented with a 12-month history of a slowly growing midline neck swelling. There were no associated aero-digestive symptoms, relevant occupational or social history.

The appearance of suprasternal midline neck lump pre Valsalva manoeuvre.

The midline neck lump is more prominent at Valsalva manoeuvre.
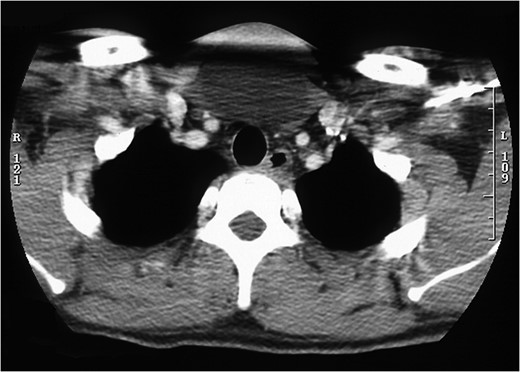
Cross-sectional image of midline neck lump with no tracheal communication.
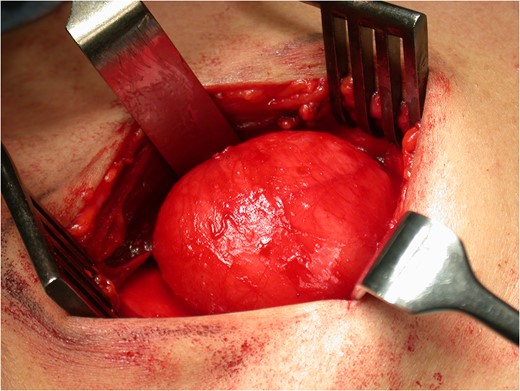
Intra-operative image of bronchogenic cyst prior to surgical excision.
DISCUSSION
Bronchogenic cysts, also known as foregut duplication cysts, are uncommon, benign, congenital lesions representing accessory bronchial buds. These cysts are found predominately in men (M:F ratio 4:1) with a prevalence of 1 in 42 000 to 1 in 68 000 [1, 2].
The cysts arise due to an abnormal budding of the ventral foregut (the future tracheobronchial tree) during lungs development. If these abnormal buds are resorbed, no further clinical sequelae arise. However, persistent buds may migrate during the course of development and rest in intrathoracic or extrathoracic region. The intrathoracic location is the mediastinum, percaridum, diaphragm and lungs while the extrathoracic site is the abdomen, oesophagus, the retroperitoneum, the subcutaneous tissue or the neck. In terms of the head and neck region, cysts can be in the suprasternal notch, presternum, shoulder, intraoral, infraclavicular region, posterior pharyngeal wall or extend into the mediastinum. A superficial presternal or suprasternal location is most common, while deep or lateral neck bronchogenic cysts are rare. Intra-dural extramedullary bronchogenic cysts in the high and mid cervical region are reported. Bronchogenic cysts are classified by Maier according to their site of origin into paratracheal, carinal, hilar, paraoesophageal, and atypical such as diaphragmatic, abdominal, intracutaneous, subcutaneous, or subscapular [3–7].
The course of upward migration begins around the carina and extends upwards either parallel to the trachea deep into the neck or towards the skin superficially. Superficial migration, similar to our case, is explained by tracheal bud development around the fifth week of development when the right and left mesenchymal bars displace the cyst anteriorly prior to their fusion. Consequently, abnormal budding during the development of the trachea may result in a midline cervical cyst whereas a lateral neck cyst may form during the development of the bronchial system. The localization of the cyst in the cervical region therefore suggests that the anomaly occurred before the fifth week of gestation. About 70% of more than the total 70 reported cases of cervical bronchogenic cysts are in the midline region. Bronchogenic cysts of the lateral neck are located in lower cervical regions whereas the upper cervical cysts are generally on the midline [8–11].
The histological finding of respiratory epithelium alone would not be sufficient to diagnose bronchogenic cysts as the same may be expected in laryngocoeles. The most reliable criterion for the diagnosis of bronchogenic cysts has been the presence of cartilage plates in the wall of the cyst, with submucosal glands and smooth muscles [12, 13].
Early surgical intervention can prevent future symptoms and complications, which may make subsequent resection more challenging. If left untreated, bronchogenic cysts may undergo squamous metaplasia, inflammation, or mucosal necrosis and thus complicate diagnostic confirmation. Furthermore, deep cysts may become infected and present as a neck abscess. The importance of resecting extrathoracic superficial bronchogenic cysts has been highlighted in a number of cases, reporting mucoepidermoid carcinoma or recurrent malignant melanoma transformation as potential complications [14–18].
The differential spectrum of a midline neck mass include thyroglossal cysts, branchial cleft cysts or thymic cysts. Unlike branchial cysts or thyroglossal cysts, bronchogenic cysts can track towards the sternal notch or have a cranial extension. Other differentials for neck cysts include cystic lymphatic or vascular malformations, lipomas, thyroid cysts, teratomas, epidermoid cysts and cystic norinomas. The clinical presentation and histological nature of these cysts is distinct from bronchogenic cysts [19, 20].
The expansile nature of the presented rare midline neck lump suggested a top differential diagnosis of an external laryngocoele due to the distinguished typical presentation superior to the laryngeal cartilage after passing through the thyrohyoid membrane. While bronchogenic cysts have not previously been described as mimicking laryngocoeles, a previous case of a lipoma presenting as a midline neck lump with shape change during valsalva manoeuvre was reported previously [21].
The pre-operative diagnosis of bronchogenic cysts based on history and imaging were only accurately made in a third of intrathoracic cases [22]. This case of bronchogenic cyst was diagnosed based on combined histological, clinical and radiological findings.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}