





Abstract
Gallbladder perforation with subsequent gallstone spillage can occur with higher frequency in laparoscopic cholecystectomy than in traditional open approach. Gallstone abscess formation from stone spillage post-cholecystectomy is extremely rare. We present a case of para-spinal abscess formation 5 years after spilled gallstones following laparoscopic cholecystectomy.
INTRODUCTION
Laparoscopic cholecystectomy (LC) is recognized as the gold standard method for treating symptomatic gallstone disease. Gallbladder perforation with subsequent gallstone spillage can occur with higher frequency in LC than in traditional open approach [1]. Stone spillage during LC is reported in the range of 5–40% of procedures [2]. These stones are usually benign but can migrate to various sites leading to complications said to occur in 0.08–0.3% of patients [2]. Gallstone abscess following spilled gallstones is a particularly rare delayed complication of LC. We report an unusual case of a 79-year-old lady who presented with a lumbar lump 5 years after undergoing LC. Subsequent imaging revealed the presence of a para-spinal abscess resulting from retained gallstones. This lady then underwent exploration of the lumbar lump and drainage of abscess on two separate occasions.
CASE REPORT
Mrs H is a 79-year-old lady who presented to her General Practitioner in March 2013 with a history of a painful and firm lump on her right flank. She was otherwise afebrile with normal vital signs. Blood tests around this time were unremarkable with a HB of 12.5, WCC of 7.9 a mildly raised ESR of 46 and otherwise normal liver/kidney function tests.

CT scan of abdomen showing soft tissue mass posterior to liver.
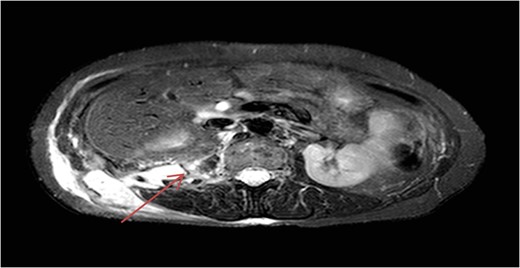
MRI of abdomen showing right retroperitoneal collection extending into right flank.
Her symptoms had been managed conservatively until re-presenting 3 years later with a back (lumbar) lump. Due to the uncertainty over the nature of this back lump, a CT and magnetic resonance image (MRI) of the abdomen was carried out. This revealed an abnormal 6.2 × 3.1 × 11.4 cm3 retroperitoneal collection extending from the posterior right edge of the liver until passing through the abdominal wall to form the palpable mass in the right flank (Figs 1 and 2).
Mrs H consequently underwent exploration of the lumbar lump and drainage of abscess in June 2013. After ongoing symptoms, an interval CT scan was carried out which showed a persistent collection. Mrs H then underwent a laying open of infected back sinus and removal of gallstone from the cavity in June 2015.
DISCUSSION
LC is recognized as the gold standard method of treatment for symptomatic gallstone disease. With morbidity rates ranging from 2 to 11% for LC compared to 4–6% for elective open cholecystectomy [3]. The benefits of LC includes; reduced mortality rates in the perioperative period, smaller period of hospitalization, faster recovery and improved cosmesis; when compared to open cholecystectomy. However, LC is not without complications and Gallbladder perforation with subsequent gallstone spillage can occur with higher frequency in LC than in traditional open approach [4]. Spilled gallstones are also removed with comparative ease in open cholecystectomy by irrigation and suction whilst this is more difficult to achieve in LC [1].
Complications initiated by stone spillage post-cholecystectomy are extremely rare and can present months or years after the cholecystectomy. Abdominal wall abscess and intra-abdominal abscesses are the most common complications from stone spillage [1]. Other potential stone-related complications include adhesions, fistula, obstruction, intestinal perforation and pleural empyema [1]. As can be seen in our case, patients presenting with an abscess can often be afebrile and have a normal white cell count. If significant stones are seen on imaging investigations during the initial presentation, it ought to be dealt with promptly, as symptomatic stones will unlikely resolve spontaneously. Management of an abscess due to spilled gallstones includes open or radiological drainage and intravenous antibiotics. Moreover, removal of spilled gallstones is considered universally important to prevent recurrence [1]. Management with laparoscopic drainage and stone removal is also feasible for certain patients [1].
Every attempt should be made in preventing stone spillage and removing all visible stones at the time of surgery. Papasavas et al. [5] described a sequence of ploys that should help with stone removal after spillage. The vast majority of authors have concluded that there is no indication for routine conversion to open surgery to retrieve spilled stones [6].
CONCLUSION
Gallstone abscess formation from stone spillage post-cholecystectomy is extremely rare. In our case, the history of LC 5 years prior, along with the finding of a retroperitoneal mass containing gallstones at surgery made the challenging diagnosis possible. The case underlines the significance of bearing in mind the complication of spilled stones when an abscess or fistula forms a number of years post surgery.
FINANCIAL SUPPORT
None.
CONFLICT OF INTEREST
None.

{kind=link}