





Abstract
Intussusception in adults lacks specific symptoms and is often diagnosed emergently when they present with obstruction. Though intussusception certainly varies in size and location, the increased likelihood of ischemia or obstruction make large intussusceptions very rare in the literature. A patient admitted to our facility for small bowel obstruction was found to have extensive intussusception from the right lower quadrant to the splenic flexure, where a lead point was identified. Histopathology revealed multiple satellite lesions surrounding the lead point tumor, which was found to be invasive mucinous adenocarcinoma of the ileocecal valve. While malignancy is found in 60% of lead point identifiable adult intussusceptions, a malignancy is always found in the case of an exceptionally large intussusception.
INTRODUCTION
Intussusception has classically been described as a childhood condition and a rarity in adults [1]. The overall annual incidence of intussusception in adults in the general population has been reported to be as low as 2 cases/1 000 000 persons; adults account for ~5% of confirmed intussusceptions. As high as 90% of cases of adult intussusception are due to a pathological process, with neoplasms accounting for ~60% of identifiable leadpoints [2]. One 6-year prospective study encompassing screening of 380 999 computed tomography (CT) scan reports that were read as intussusception, 0.04% of cases were in adults [3]. In adults, surgery is typically performed owing to the likelihood that a neoplastic or otherwise chronic pathology is the cause of the intussusception [1]. Indications to take any case to the operating room include large caliber of telescoped bowel, long length of telescoped portion, identifiable lead point and evidence of obstruction [2–4]. The former indications owe to the increased likelihood of malignancy requiring surgical exploration and incision, and bowel wall and mesenteric ischemia in the setting of large intussusceptions [4].
CASE REPORT
A 61-year-old gentleman presented with a 3-day history of right-greater-than-left lower quadrant abdominal pain, distention, anorexia and one episode of emesis. The patient also reported only consuming liquids for 5–7 days prior to presentation as solid foods caused significant discomfort. He endorsed intermittent cramping in the past year with a 20-lb unintentional weight loss. Three weeks prior, colonoscopic evaluation of his cramping was aborted at 20 cm due to an impassable sigmoid stricture. Several hyperplastic polyps and one tubular adenoma were removed at that time.
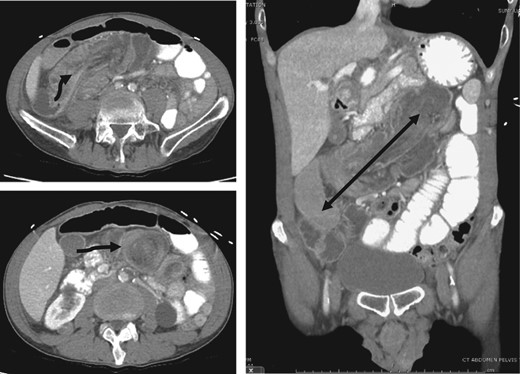
Top left: origin (arrow) of invagination in the right lower quadrant. Bottom left: the classic ‘target sign’ (arrow). (Right) Coronal demonstrating the extent of intussusception.
SURGERY AND PATHOLOGY

Left: stills from intraoperative video recording demonstrating the reduction of the intussusception in order to explore the lead point. Right: ischemic terminal ileum (arrow) and palpation of the lead point at the ileocecal valve.
![Low-power (left) and high-power (right) views of lead point tumor demonstrates >50% of the tumor composed of pools of mucin (solid arrow), invasive tumor cells (dotted arrow) with hyperchromatic chromatin, crowded nuclei, surrounded by pools of mucin [5–7].](https://oupdevcdn.silverchair-staging.com/oup/backfile/Content_public/Journal/jscr/2017/3/10.1093_jscr_rjx030/8/m_rjx030f03.jpeg?Expires=1785820080&Signature=XViMZQoW8OJMp0638Pma5X-8QuO2aDgSGqu3GWE1VOq1ivJ855J2jBs1PipQagPDIJJmS5SzoHjYhh-IJWRvxNwhApH16lvUSwMmK9tvfBktLF1kVnG4iHxGAW8SVRZH4KX8rZEwPIAn5Qzy1aazIDpGyo3IduDiR-pOLsvXqM90PCi1vMzpjOkw~rVxumJQQg07sH6EJRqFEF51xS2bsDater0gw6Ym3fo7bEww~QZ1f1OjupvMXA25bwDfNJUK3zH5ie0o8ul2AdTnS1dulUE5CtFgkslJ-tsH5mKe9kngu6ojp9QTj1gEouzEIUotkbeaVIDfVgRwH-Ck0FU8nQ__&Key-Pair-Id=APKAIYYTVHKX7JZB5EAA)
DISCUSSION
This patient's presentation is exceptionally unique for both the size and cause of intussusception. To our knowledge, very few case reports have ever described such a long-tract intussusception. The few cases we found were always in the setting of malignancy, the patients presented with a similar chronologic progression with escalation of symptoms including liquid-only diets shortly before presentation. Additionally, the very large intussusceptions were always found in the setting of malignancy [10–12]. It seems that a favorable (mobile) anatomy with an indolent process is a common thread amongst these rare cases.
Further compounding the uniqueness of this case is the lead point tumor's location and histology, along with the presence of additional terminal ileum and colonic polyps. The annual incidence in the United States of small bowel adenocarcinoma from 1973--2005 is 6.8 cases per 1,000,000 person years, as calculated by Surveillance Epidemiology and Results (SEER) program. Additionally, ileocecal adenocarcinoma of any type is sparsely described outside of a few case reports [8, 9, 13–15]. Mucinous adenocarcinoma tends to be a locally aggressive tumor, and metastasizes by redistribution phenomenon rather than vascular or lymphatic invasion. Pseudomyxoma peritoneii, or ‘jelly belly,’ is a rare complication [16].
Presently, we have no unifying diagnosis to correlate the multiple lesions found throughout the telescoped bowel and distal 20 cm of colon and rectum. However, it is currently estimated that up to 40% of patients with extensive polyps and a positive family history are ruled out for HNPCC by genetic testing for mismatch repair and MSI, as was the case for this patient [17]. Nevertheless, the unique presentation of this patient allowed for expeditious removal of a classically aggressive tumor, in what appears to be the first reported case of a long-tract intussusception secondary to a mucinous adenocarcinoma of the ileocecal valve.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}