





Abstract
Klippel–Trenaunay syndrome (KTS) is a vascular lymphatic malformation underlying with bony and soft tissue hypertrophy. It is a rare condition presenting in 1 out of 10 000 people. The growth disturbance due to KTS is more commonly unilateral (85%) than bilateral (12.5%), and most rarely crossed-bilateral (2.5%). A man in his 40s presented to our hospital with a complaint of lower limb discomfort. Radiograph, ultrasonography, computed tomography venography, magnetic resonance (and venography) showed various radiological findings characteristic for KTS. Because the patient was symptomatic, he underwent stripping of bilateral great saphenous vein and varicectomy of bilateral legs. The surgical procedures were undertaken successfully, and there has been no recurrent symptom for about 2 years and a half. In this study, we report a very rare case of bilateral KTS diagnosed by radiological and clinical manifestations with some literature review.
INTRODUCTION
Klippel–Trenaunay syndrome (KTS) is a rare congenital vascular malformation disease commonly associated with the overgrowth of bone or soft tissue [1]. Most KTS's are unilateral distribution, and bilateral distribution is very rare [2]. We describe a very rare case of KTS presenting in bilateral lower limbs confirmed with radiological and clinical findings.
Case Report
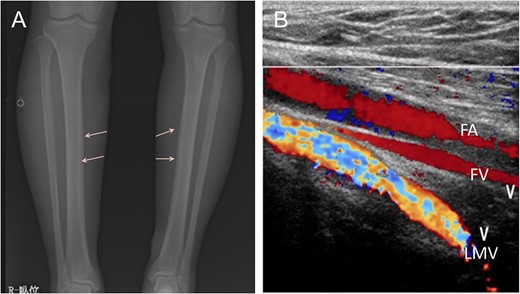
Radiograph showed bone cortex hypertrophy (arrow) of the lower limbs (A). Dilation of superficial vein in bilateral lower limbs, retrograde flow of bilateral great saphenous vein and persistence of the lateral marginal vein were detected by ultrasonography. FA, femoral artery; FV, femoral vein; LMV, lateral marginal vein (B).
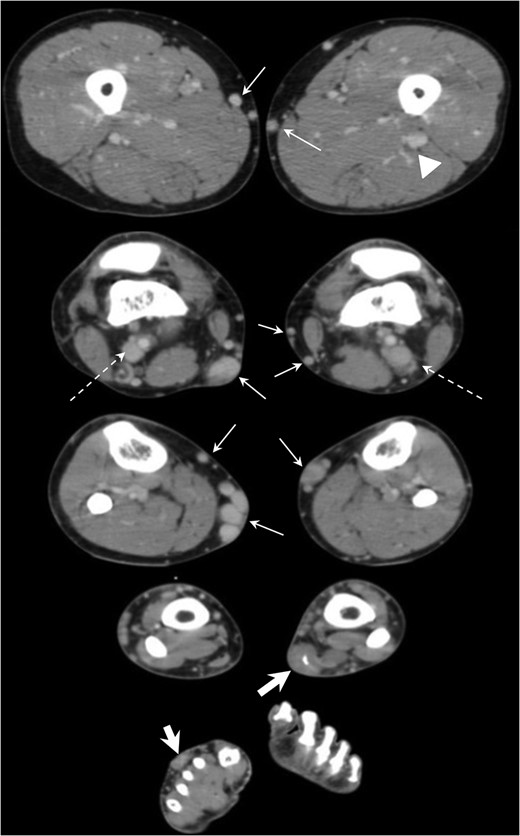
CT venography revealed dilation of superficial veins in bilateral lower limbs (arrows), persistent with the bilateral lateral marginal veins (dotted arrows) and left sciatic vein (arrow head) and soft tissue density area centered in dorsal subcutaneous fat layer of right foot and left lower limb (thick arrows).
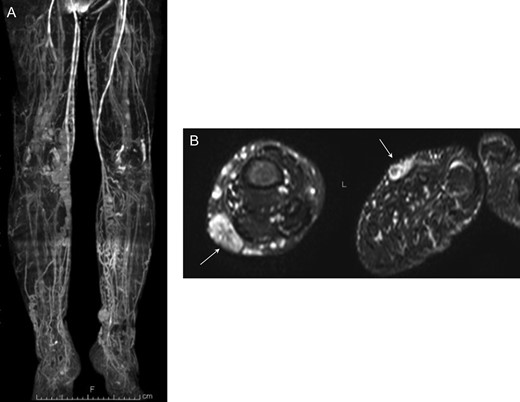
MR venography confirmed dilation of superficial lower limb veins (A). STIR MR imaging detected high signal intensity mass (arrows) indicating multiple lymphovascular malformation in subcutaneous fat layer of bilateral feet (B).
These characteristic radiological findings were compatible with the diagnosis of KTS. The patient underwent stripping of bilateral great saphenous vein and varicectomy of bilateral legs. The surgeries underwent successfully, without postoperative complications. There has been no recurrent symptom for about 2 years and a half.
DISCUSSION
KTS was first described by Klippel and Trenaunay in 1900 as vascular lymphatic malformation underlying bony and soft tissue hypertrophy [1]. It is a rare condition presenting in 1 out of 10 000 people with no gender preference [2]. The clinical presentation due to KTS is more commonly unilateral (85%) than bilateral (12.5%), with remaining 2.5% being crossed-bilateral (i.e. right upper extremity and left lower extremity) [2]. These lesions are presenting most frequently in the anterolateral and medial aspects of the calf or thigh [3]. Presenting symptoms and manifestations include pain, discomfort, leg length discrepancy, erysipelas, venous thrombosis, pulmonary embolism and/or gastrointestinal bleeding [4].
This entity is classified as combined vascular malformation type [2, 4], also as capillary—venous—(± lymphatic) malformation with limb overgrowth in ISSAVA classification [5]. The diagnosis can be made if two of the following findings are present: hypertrophy of the soft tissue and bone overgrowth, capillary hemangioma, and/or underlying diffuse venous and lymphatic malformations [6]. In this case, radiograph, CT and magnetic resonance imaging showed hypertrophy of cortical bone overgrowth and diffuse venous and lymphatic malformations in bilateral lower legs, compatible with KTS. One of the most characteristic findings of KTS is the presence of remnant embryonic veins of the superficial venous system presenting as lateral marginal vein or sciatic vein [4], which were seen in this case on ultrasound and CT. Varicose veins or anomalous lateral veins and venous malformations are observed in 68–80%, and sciatic vein involvement has also been described in KTS [6, 7].
Etiology of this entity is unknown. There is a discussion on its relevancy to vessel gene VG5Q mutation of short arm of chromosome [2]. Some suggested mechanisms include primary obstruction of the venous system resulting in venous hypertension, failure of regression of the lateral limb bud vein and changes of angiogenesis, and vasculogenesis because of numerous genes [7].
Imaging investigations are powerful for diagnosis of KTS [2]. Radiograph is most helpful to measure bone morphology, the characteristic finding of KTS [7]. Phlebography is naturally considered useful as it is a venous malformation [2, 6]. Ultrasonography is known as useful modality to assess the vascular patency, incompetence, thrombosis, arteriovenous shunting and any anomalies such as hypoplasia of veins [6]. CT venography and MR venography can be useful to evaluate deep venous system and dilated superficial and embryonic veins [4, 6].
Conservative management is often recommended [7]. Compression therapy has been performed when both lymphedema and chronic venous insufficiency are present [2, 7]. There are also some invasive managements; pulse dye laser therapy for port wine stain, YAG laser for very superficial vein, serial sclerotherapy with absolute alcohol and foam sclerotherapy [2, 7]. In some cases, recurrent deep vein thrombosis can happen as a result of cellulitis and lymphangitis, anticoagulation or inferior vena cava filters are utilized in such cases and for the purpose of pulmonary embolism prevention [8]. Surgeries are reserved for symptomatic patients and must be preceded by careful evaluation of the extent of malformations and patency of the deep system [7]. Complete surgical resection of the marginal vein is considered one of the treatment choices if normal deep veins are maintained [7]. Vascular intervention treatments are rarely performed [6].
CONCLUSION
The diagnosis of KTS presenting with bilateral lower limbs may be challenging because of the low incidence. However, the correct diagnosis can be reached with properly performed imaging studies along with the history, which leads to appropriate treatment.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}