





Abstract
A 21-year-old male involved in a motorcycle crash presented with abdominal hemorrhage and a widened mediastinum on chest radiograph. He required an initial exploratory laparotomy for mesenteric injuries. An aortic injury was confirmed on computed tomography imaging and he subsequently underwent attempted endovascular repair. During that procedure, the patient experienced massive thoracic hemorrhage with cardiac arrest and profound respiratory failure. Damage-control thoracic surgery and rescue extracorporeal membrane oxygenation were successfully utilized with a favorable outcome.
INTRODUCTION
Traumatic aortic injuries occur with severe deceleration type injuries [1]. Contemporary management involves rapid diagnosis, treatment of associated injuries and endovascular treatment [2]. Extracorporeal membrane oxygenation (ECMO) is available at some centers for refractory cardiac and respiratory failure and has been used in the trauma setting [3]. We report a case of emergent rescue application of ECMO in a patient with profound cardiac and respiratory failure during endovascular repair of an aortic rupture.
CASE REPORT
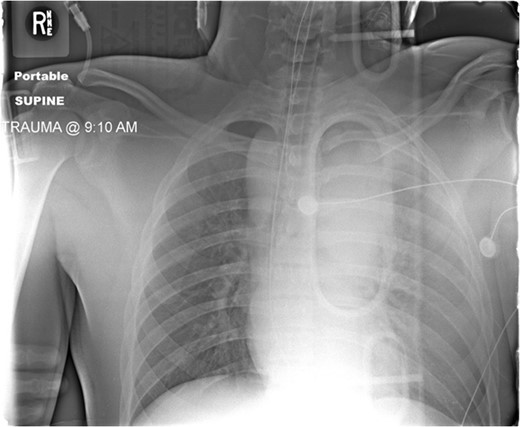
Admission AP CXR demonstrating a widened mediastinum and increased haziness of the left hemi-thorax.
During the abdominal exploration, multiple mesenteric injuries were identified and repaired. An abbreviated damage control laparotomy with packing was performed. A left-sided chest tube was inserted and drained ~800 ml of blood without continued hemorrhage.
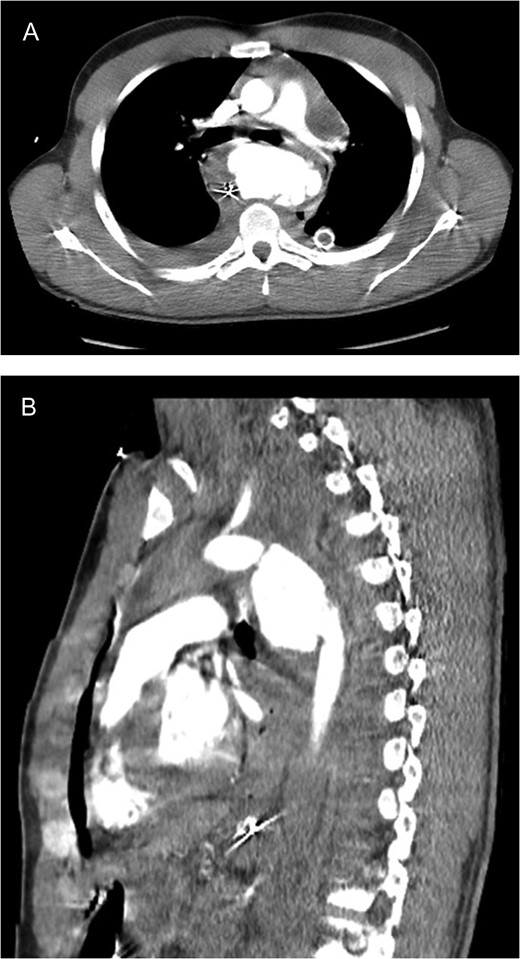
CT scan images (A axial; B sagittal) demonstrating aortic rupture with active contrast extravasation at the level of the proximal descending aorta just distal to the ductus on both axial and sagittal imaging.
Bilateral femoral arteries were accessed and an aortic endovascular stent was deployed to cover the area of injury. During the procedure, the patient developed significant hemorrhage from the left chest and became hypotensive. An emergent left thoracotomy was performed and the mediastinum was packed temporarily while the vascular team deployed an additional two stents over the area of injury, including the origin of the left subclavian artery. This resulted in exclusion of the aortic injury with no signs of radiographic leak.
The patient required massive transfusion resuscitation and cardiopulmonary resuscitation was performed for the exsanguinating hemorrhage. The patient had multiple episodes of cardiac arrest and required internal defibrillation as well. Due to persistent severe cardiac and respiratory failure, the cardiac surgeons placed the patient on veno–arterial ECMO emergently. The hemorrhage from the chest was controlled with packing. The patient remained very unstable and subsequently required an additional venous cannula in the right internal jugular vein. The resultant veno–veno–arterial (VVA) ECMO finally improved his oxygenation. Flows were adjusted in order to maintain adequate oxygenation. The abdomen required open decompression and was managed with a temporary abdominal dressing. He was transferred to the intensive care unit in very critical condition.
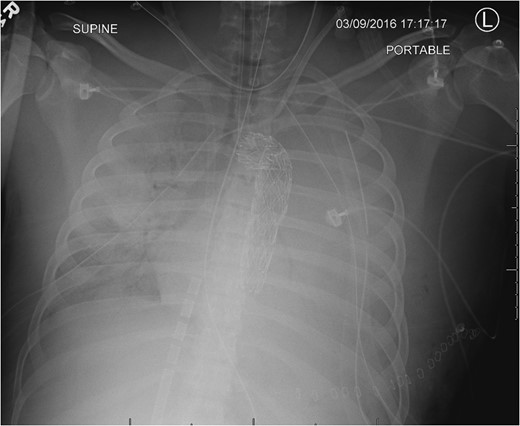
CXR following chest closure on postop day 3 demonstrated the aortic stent, multiple life support lines and bilateral lung opacification from the severe persistent respiratory failure.
He slowly improved and by postop day 11, the ECMO cannulas were discontinued. He later developed a pericardial effusion which required open drainage (postop day 18); however, the respiratory and renal failure eventually resolved. He later required surgery on his left hand fracture and subsequent debridement of the left groin. He was transferred to inpatient rehab on hospital day 35 and was discharged home by hospital day 44 without gross neurologic sequela.
DISCUSSION
Traumatic rupture of the aorta is an uncommon, yet lethal injury. Most deaths occur at the scene of the trauma [4]. The most common mechanism for an aortic injury is from a motor vehicle crash. Only 10–20% of patients with aortic injury survive to hospital arrival [4]. Most injuries are associated with a deceleration type mechanism and are usually located at a fixed location of the aorta near the isthmus just distal to the left subclavian artery. Associated injuries are common and contribute to morbidity and mortality [1].
For patients surviving to hospital arrival, aortic rupture is suspected when a widened mediastinum is observed on the initial CXR and later confirmed with angiographic imaging [1]. CTA is the current test of choice in a trauma patient with suspicion of aortic injury [5]. Once injury is diagnosed, strict blood pressure and heart rate control are instituted in order to decrease shear stress on the contained rupture [5]. Aortic endovascular stent grafting has become the most common treatment technique [6]. Short-term results and outcomes show less overall mortality and paraplegia than an operative approach through thoracotomy [2].
Previously, ECMO has been reported as a rescue therapy option in cases of severe respiratory failure in trauma patients [3, 7, 8]. In addition, ECMO has also been described in the management of patients with aortic injuries [9, 10]. Our patient, however, received emergent rescue ECMO during cardiac arrest due to exsanguinating hemorrhage during aortic stent graft repair. Damage-control thoracic surgery allowed deployment of additional stents when the patient became unstable with massive chest hemorrhage. In addition, our patient required a second return venous cannula to improve oxygenation beyond the single venous return from the oxygenator. Remarkably, he survived the cardiac arrest and shock without gross neurological compromise.
Our case exemplifies the multi-disciplinary approach required to treat a complex aortic injury with massive hemorrhage. Damage control techniques and rescue ECMO therapy during cardiac arrest resulted in survival from an otherwise fatal injury. Application of ECMO for acute heart and lung failure after massive hemorrhage and resuscitation remains institution dependent but could be applied in certain circumstances.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}