





Abstract
Giant phyllodes tumors (PT) are an uncommon fibroepithelial neoplasm and especially rare in adolescent girls. Diagnosis is difficult not only due to the rarity of PT, but also owing to the resemblance of its clinical and imaging features with fibroadenoma. The author reports a case of a giant PT in a 14-year-old girl. Clinical examination showed a large painful mass in the left breast, and an abscess was initially suspected. But magnetic resonance imaging (MRI) displayed features characteristic of PT. Following complete surgical excision of the mass, histopathology confirmed the diagnosis of a benign PT with diffuse myxoid changes, consistent with the MRI findings. This case emphasizes the importance of breast MRI, both for its ability to aid diagnosis, as well as its benefits in guiding the surgical plan.
INTRODUCTION
Palpable breast masses are uncommon in pediatric and adolescent populations; when they do occur, they are most often benign in nature such as secondary to normal developmental changes or benign neoplasms. Despite generally being benign, they require medical attention when the mass is due to infection, or displays a rapid increase in size [1, 2]. Diagnosis and treatment of such cases in adolescents must be appropriately tailored to avoid damage to the developing breast tissue, which may result in hypoplasia or aplasia [2]. Ultrasound (US) is the primary imaging modality used in young patients during the initial diagnosis, assisting in imaging-guided biopsy when indicated, magnetic resonance imaging (MRI) of the breast is rarely performed [2]. But in large mass, there are some limitations of US to accurately evaluate the extent, margin and relationship of the mass with surrounding normal tissue. Herein, the author describes a case of a giant phyllodes tumor (PT) diagnosed in an adolescent girl, and the role of breast MRI in determining the diagnosis as well as in planning for the appropriate approach for breast conservation surgery.
CASE REPORT
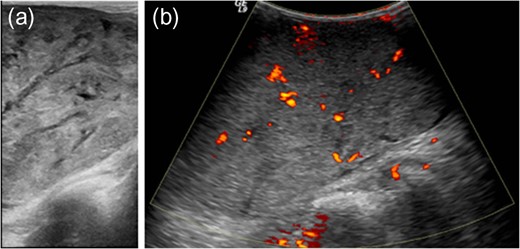
Gray-scale ultrasound shows a circumscribed, solid mass with heterogeneous internal echotextures, including hyperechoic, hypoechoic and multifocal anechoic areas, some of which were linear cleft-like in shape (a) and the color Doppler sonography demonstrates increased intralesional vascularity (b).
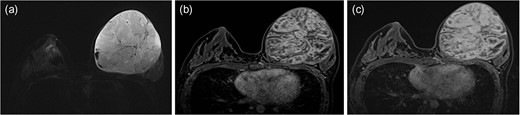
Axial STIR image of breast MRI shows a well-circumscribed mass with heterogeneous signal intensities (SIs), consisting of solid components with iso-to-high SIs, with interspersed by areas of cystic portions. These cystic areas are also noted along the periphery of the mass. Dark focal SI due to hemorrhage and signal voids due to fast flowing blood vessels are seen (a). On dynamic contrast-enhanced T1WI, the solid portions shows early intense heterogeneous enhancement on 1 min image (b) with a persistent pattern on the late phase of 5 min image after contrast administration (c).
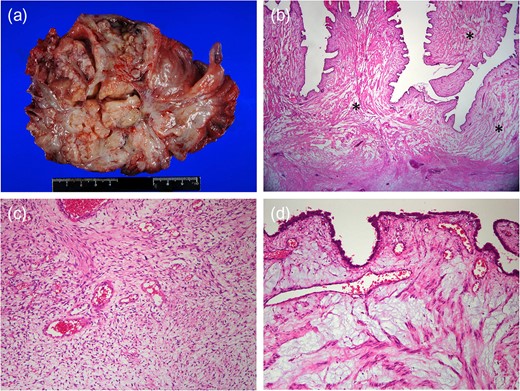
Gross specimen reveals myxoid and friable on sectioning (a). Low-power magnification demonstrates cellular stromal component and characteristic leaf-like projections into cleft-like spaces (H&E, ×10). Stromal component shows extensive myxoid change (asterisks) (b). The central non-myxoid area shows mild hypercellularity and mild nuclear atypia, typical features of benign phyllodes tumor (H&E, ×100) (c). Prominent myxoid changes of the stroma are seen in many areas (H&E, 100) (d).
DISCUSSION
PT is rare fibroepithelial lesion accounting for <1% of all breast neoplasms. The median age of diagnosis is 45 years, and it is rare in adolescents. There is a higher incidence of PT in Asian heritage [2, 3]. Histologically, they may be classified as either benign, borderline and malignant. Most PTs are benign (63–78%), with borderline PTs diagnosed in only 11–30% of cases. Based on clinical, radiological and cytological examination, PTs are often indistinguishable from fibroadenomas, the most common breast mass in adolescents [3, 4].
In the case of a rapidly growing mass, an uncommon histologic variant of fibroadenoma (juvenile or cellular) may be difficult to differentiate from PT based on clinical parameters, imaging features and even though core biopsy. Differentiation between these two neoplasms is dependent on histologic examination of the excised tumor [5, 6]. Findings such as cystic components, distinct lobulations and heterogeneity on delayed contrast enhancement are suggestive of PT on breast MRI [5, 7, 8]. In this case, the characteristic features like cleft-like cystic spaces and heterogeneous enhancement on delayed phase were essential to make a presumptive diagnosis of PT.
We also noted the unusual finding of diffuse myxoid changes on histopathologic examination. Myxoid change in the stroma of PT tends to be patchy and to undergo degenerative changes; focal stromal myxoid change is not uncommon in a benign PT, but a tumor composed diffusely of this tissue is very unusual [9]. These diffuse changes might have contributed to the heterogeneous SIs on breast MRI with cystic or hemorrhagic necrosis.
In adults, PTs can be excised with 1-cm margins to reduce recurrence rates; in adolescents, these tumors should be excised with only a minimal rim of normal tissue to maximize breast conservation [2, 10]. For this patient, the breast MRI clearly delineated the margin of the mass, allowing for easy dissection of the mass from the chest wall and normal surrounding glandular tissue. Without this information, breast conservation surgery could not have been performed effectively. In adolescents, US is the imaging modality of choice for mass evaluation. However, if the lesion is very large or sonography is insufficient to characterize the lesion, contrast-enhanced MRI could depict the more specific natures of the lesion.
Although the incidence is very low, and it is indistinguishable from the more prevalent fibroadenoma in this age group, PT should be considered if MRI reveals the characteristic heterogeneous features. Moreover, high tissue contrast provided by MRI can assist greatly in visualizing the relationship of the lesion to normal structure, helping the surgical team conservation as much health tissue as possible during the excision.
CONFLICT OF INTEREST STATEMENT
None declared.
FUNDING SOURCES
None.

{kind=link}