





Abstract
Cystic lymphangiomas of the mesocolon are very rare in adults. They are usually asymptomatic, but can present with an acute abdomen. We report an adult patient with cystic lymphangioma of the mesocolon that manifested with peritonitis. A 33-year-old man presented with fever and severe pain with muscle guarding in the left abdomen. Laboratory data indicated high-grade inflammation. Enhanced computed tomography (CT) showed multiple low-density masses with peripherally enhancing rims, strongly suspicious for cysts, in the left abdomen. Based on a diagnosis of peritonitis, emergency surgery was performed and revealed many cysts in the descending mesocolon. Histopathological examination findings indicated a cystic lymphangioma. The post-operative course was uneventful, and 1-year follow-up CT showed no recurrence. This case demonstrates that cystic lymphangiomas of the mesocolon in adults can present with acute peritonitis, although this is extremely rare. Complete resection is required for accurate diagnosis and for preventing recurrence.
INTRODUCTION
Acute abdomen can have many causes and often requires surgery for definitive diagnosis. Cystic lymphangiomas are uncommon benign tumours considered lymphatic system malformations [1]. These are usually found in the head, neck and axilla in children, and are most commonly asymptomatic and discovered incidentally [2, 3]. Cystic lymphangiomas arising from the mesocolon are rare in adults and seldom present with acute abdomen. Treatment varies from conservative therapy to complete resection [1, 2]. We report a case of cystic lymphangioma of the mesocolon presenting with peritonitis, in which emergency surgery was performed successfully.
CASE REPORT
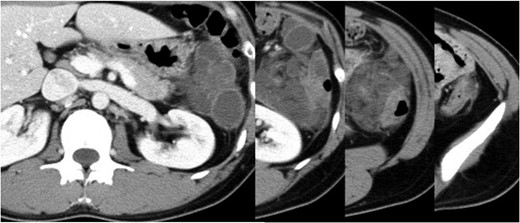
Abdominal enhanced CT showing multiple cysts with inflammation in the descending mesocolon.

Intraoperative findings on laparotomy. Multiple blueberry-coloured cysts were identified in the descending mesocolon.
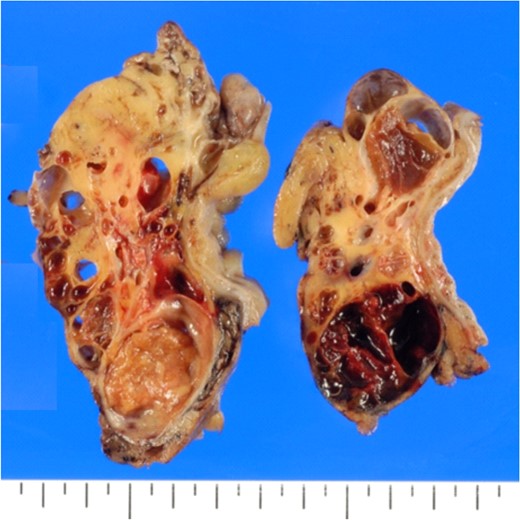
Cut surfaces of the cystic lesions showing a multi-cystic space with recent haemorrhage and suppurative inflammation.
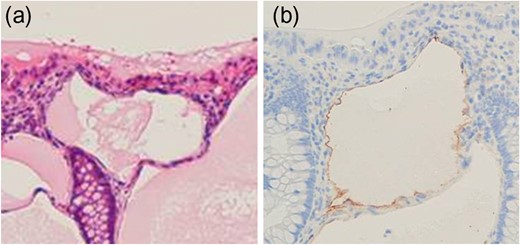
(a) Dilated tubules lined by flat cells. (b) Immunostaining for podoplanin/clone D2-40. The flat cells express podoplanin.
The patient's post-operative course was very good, and the patient was discharged on the 15th post-operative day. A 1-year follow-up showed no symptoms or recurrence.
DISCUSSION
We report a rare case of cystic lymphangioma of the mesocolon. Cystic lymphangiomas of the mesocolon can present with acute abdominal symptoms such as peritonitis, although most are asymptomatic. Complete resection is the most definitive treatment for diagnosis and avoiding recurrence.
Lymphangiomas are very rare; the incidence is ~1 case per 20 000 paediatric patients admitted to hospital [1]. Lymphangiomas at any location account for ~5–6% of all benign tumours in children [2]. They most commonly occur in children, and rarely in adults. A total of 90% of lymphangiomas occur in the head, neck and axilla; intra-abdominal lesions are very uncommon and account for <5% of lymphangiomas [3]. The mesentery of the small bowel is the most common location of intra-abdominal lymphangiomas, followed by the omentum, mesocolon and retroperitoneum [2]. Right mesocolonic lesions are more frequent than left lesions [4].
The aetiology of lymphangiomas remains unclear. The most well established theory suggests that lymphangiomas arise from congenital anomalies of the lymphatic system. This theory is supported by the fact that most lymphangiomas occur in children [5, 6]. Another theory is that these lesions develop in response to stimuli, such as inflammation, abdominal trauma, surgery or radiation therapy [6]. In our case, the patient had no history of abdominal surgery or disease; therefore, other mechanisms may exist.
Mesenteric and mesocolonic lymphangiomas are usually asymptomatic; any related symptoms are variable and non-specific, depending on the lesion size and location, although a palpable abdominal mass and abdominal distension are most common [4, 6]. Intra-abdominal cystic lymphangiomas infrequently present with acute abdomen, including bowel obstruction, volvulus, bleeding and infection [7]. In total, 90% of lymphangiomas become symptomatic before a mean age of 2 years [1]; therefore, it is uncommon for cystic lymphangiomas of the mesocolon to cause severe, life-threatening abdominal symptoms in adults [8]. The chief symptom in our case was severe abdominal pain with signs of peritoneal irritation due to inflamed cystic lymphangiomas. Ultrasonography (US) is an appropriate modality for evaluating acute abdomen and it is valuable for diagnosing cystic lesions [2, 7]. However, CT and magnetic resonance imaging (MRI) are superior to US in terms of providing detailed information about lesion size, location and extent of spread [8]. MRI provides more precise differentiation from other cystic-like masses. However, in emergency cases, CT plays a key diagnostic role, given its wide availability and quantity of information provided [7]. Lymphangiomas of the mesocolon must be distinguished from other fluid-filled lesions, such as pseudocysts, dermoid cysts, enteric duplication cysts, lymphocoele, mesothelioma, lipoma and various types of sarcoma [9]. In our case, CT showed cystic lesions with peripherally enhancing rims and surrounding inflammation that corresponded with the painful region and were suspected to correlate with peritonitis; the differential diagnosis included lymphangiomas and other cyst-forming diseases.
Complete resection is the most definitive treatment for diagnostic confirmation and recurrence prevention. Diagnostic confirmation is difficult without surgery, although imaging can provide diagnostic information in some cases.
Incomplete resection results in a 10% post-operative recurrence rate [10]. Complete resection is essential for lymphangiomas of the mesocolon, and usually requires bowel resection.
Conservative treatment may be recommended, given the 10% chance of spontaneous regression for asymptomatic cases [2]; however, resection may be required to avoid complications related to cyst growth [8].
Recently, laparoscopic surgery was recommended for treating lymphangiomas [4]. This modality is effective if a good operative view and an experienced surgeon are available, although this is often difficult in emergency cases.
We have presented a case of cystic lymphangioma of the mesocolon with peritonitis that was successfully treated with emergency surgery. This is an infrequent cause of acute abdomen in adults, and should be distinguished from other cyst-forming entities. Complete resection is the most definitive treatment for diagnostic confirmation and recurrence prevention.
CONFLICTS OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}