





Abstract
A parastomal hernia is the abnormal protrusion of intra-abdominal tissue and organs through a defect in the abdominal wall around an ostomy. Commonly, they involve intra-abdominal fat, omentum or bowel. However, there are rare cases that involve other organs. We present the case of an 89-year-old gentleman with a gallbladder in his parastomal hernia. Due to his acute cholecystitis, the distended gallbladder compressed adjacent bowel loops in the parastomal hernia, resulting in a mechanical bowel obstruction. The patient was treated with antibiotics and a nasogastric tube. As his cholecystitis resolved his ostomy function returned.
INTRODUCTION
A parastomal hernia is the abnormal protrusion of intra-abdominal contents through a defect in the abdominal wall around an ostomy. It is rare to have a gallbladder within a parastomal hernia. Here, we describe an inflamed gallbladder within a parastomal hernia causing a bowel obstruction.
CASE REPORT
Our patient is an 89-year-old male with a history of a Hartmann’s procedure (2006) for Crohn’s disease of the sigmoid colon followed by a reversal of the colostomy with a diverting loop ileostomy (2008). Due to his comorbidities and age, the patient declined further surgery to reverse his loop ileostomy. Most recently, the patient presented to the emergency room with no ostomy output for the past 14 h, nausea and frequent burping. He reported a burning sensation around his ostomy. His physical examination revealed a large parastomal hernia in the right hemiabdomen and associated tenderness in the right upper quadrant, with no overlying skin changes. His white blood cell count was 8.1 (82.4% neutrophils), and he had normal liver function tests. A computed tomography (CT) scan of the abdomen and pelvis revealed a large parastomal hernia with a wide neck containing a distended gallbladder concerning for acute cholecystitis, as well as a small bowel obstruction with a transition point at the level of the hernia (Figs 1 and 2). A previous CT scan showed the same hernia with a nondistended gallbladder and non-obstructed bowel entering and exiting the stoma (Fig. 3).
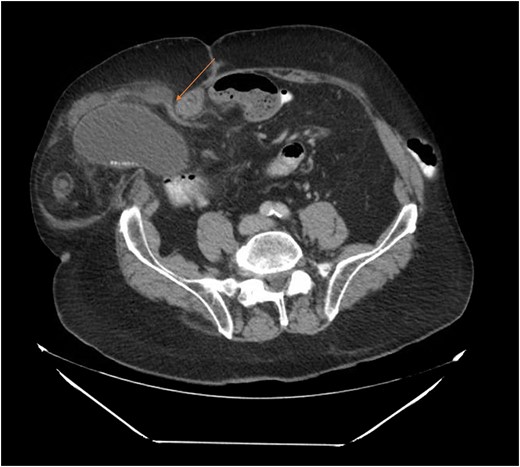
Acute cholecystitis causing a small bowel obstruction within a parastomal hernia. Arrow points to transition point.

CT from current admission with distended gallbladder consistent with acute cholecystitis.

CT from May 2017 with decompressed gallbladder and unobstructed bowel.
The patient was diagnosed with acute cholecystitis causing a small bowel obstruction within a parastomal hernia. A nasogastric tube was placed with return of 300 ml of bilious fluid. The patient was admitted and started on IV antibiotics for his acute cholecystitis. He had cardiopulmonary comorbidities and was deemed a poor surgical candidate by his cardiologist, so the patient declined any further surgeries. As his acute cholecystitis resolved with antibiotics, his ileostomy began functioning and the nasogastric tube was removed. His diet was advanced and his ostomy continued to function. His hospital course was complicated by a chronic obstructive pulmonary disease exacerbation which improved with steroids and nebulizer treatments. The patient recovered well and was discharged home on hospital day 5.
DISCUSSION
Based on a literature analysis by the British Journal of Surgery, the incidence of parastomal hernias is 1.8–28.3% for end ileostomies, 0–6.2% for loop ileostomies, 4–48% for end colostomies and 1–30.8% for loop colostomies. It is believed that loop ostomies only have lower incidence compared with end ostomies because they are more likely to be temporary, resulting in less time for a hernia to develop [1]. Surgical repair is recommended if the hernia is interfering with stoma function or the tissue becomes incarcerated in the hernia sac.
On review of the literature, parastomal hernias containing the gallbladder are extremely rare. We found only five case reports. The first involved an 88-year-old woman with rectal prolapse after a sigmoid colectomy with transverse loop colostomy who presented with fevers and abdominal pain. She was found to have a chronically inflamed, distended and thickened gallbladder in her parastomal hernia. The hernia was manually reduced and patient was discharged without a cholecystectomy because she was a poor surgical candidate [2]. The second case was an 85-year-old woman status post cystectomy for urothelial carcinoma with an ileal conduit who presented with fevers and abdominal pain. A thickened, edematous gallbladder was found in a parastomal hernia. She was taken to the operating room (OR) for an exploratory laparotomy, drainage of gallbladder and cholecystectomy [3]. The third case was a 63-year-old female status post transverse colectomy and colostomy for ischemic colitis who presented with abdominal pain, anorexia, nausea and increased ostomy output. She had a parastomal hernia containing her gallbladder, but her symptoms resolved with bowel rest and intravenous fluids. The hernia spontaneously reduced [4]. The fourth case was a 74-year-old female status post total colectomy and end ileostomy for ulcerative colitis who presented with abdominal pain and a large, tender, irreducible parastomal hernia. She went to the OR where an incarcerated gallbladder compressing small bowel was found in the hernia. The pathology showed a chronically inflamed gallbladder [5]. The final case was a 76-year-old gentleman status post total colectomy and end ileostomy for ulcerative colitis who presented with abdominal pain and a non-reducible parastomal hernia. In the operating room, they found a parastomal hernia containing a torsed gallbladder. A cholecystectomy was performed [6].
Herniation of the gallbladder is rare, as demonstrated by this literature search. After a thorough review of the literature, we believe that this is the sixth reported case of a parastomal hernia that contains the gallbladder. However, this is the only reported case where acute cholecystitis resulted in a small bowel obstruction due to mechanical compression. Our patient had a distended gallbladder consistent with acute cholecystitis on CT scan when compared with a prior CT scan where the gallbladder was seen in the parastomal hernia, but without signs of distension or inflammation. The distended gallbladder was compressing the small bowel as it entered the parastomal hernia, resulting in a small bowel obstruction without any signs of ischemia. Of note, manual reduction of the patient’s hernia was not attempted in this case given the friability of the gallbladder secondary to acute cholecystitis and the potential for gallbladder rupture.
No consensus was found on literature review regarding surgical versus medical management in patients with acute cholecystitis within a parastomal hernia. We believe this decision should be made on a patient by patient basis. In our case, one possible management option would be to surgically reverse the loop ileostomy and repair the parastomal hernia, with or without a concomitant cholecystectomy. However, as indicated previously, the patient was deemed a poor surgical candidate due to his extensive comorbidities. Therefore, the decision was made to treat the cholecystitis with antibiotics and his bowel obstruction with bowel rest and a nasogastric tube decompression. The patient understood that if conservative measures failed, more aggressive management, such as surgery or a percutaneous cholecystostomy tube, may be indicated for this condition. However, after 1 day of antibiotics and bowel rest, the patient’s condition improved and resolved without more invasive measures.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES
Author notes
Chetna Bakshi and Samantha Ruff These authors contributed equally to this work.

{kind=link}
{kind=link}
{kind=link}