





Abstract
We report a case of chronic myelomonocytic leukaemia (CMMoL) in a 68-year-old man who developed osteomyelitis of the mandible. At the initial visit, he reported uncontrolled gingival bleeding, despite self-administered haemostasis. He complained of severe pain in the socket, despite potent opioid analgesia. After consultation with the internal medicine specialists, we undertook a surgical anti-inflammatory approach that included sequestrectomy with massive blood transfusion. His physical condition was ameliorated after the surgical procedure, and he was discharged from the hospital. However, 3 months later, he died because of cardiac arrest after haemorrhagic shock and cardiovascular failure because his CMMoL had developed to an acute blastic crisis. This experience demonstrates that the most important goal in such cases is to alleviate a patient's discomfort by applying minimally invasive actions to eliminate infection and improve the quality of life without causing deterioration in the CMMoL status.
Introduction
Chronic myelomonocytic leukaemia (CMMoL) is a rare disease with an incidence of 0.37–0.72 per 100 000 population. The median age at diagnosis varies between 65 years and 75 years [1–4]. It has a 2:1 male predominance [5, 6]. The radical treatment is allogeneic stem cell transplantation, although this treatment is unsuitable for most patients because of their advanced age [6, 7]. Hence, the prognosis of CMMoL is very poor. The median survival of patients with CMMoL is 15–20 months [5, 6, 8]. Several case reports have indicated that excess surgical stress causes an acute blastic crisis, which contributes to a poor outcome [9, 10].
Case Report
A 68-year-old man complained of having a reduced appetite for approximately 5 months and weight loss during the previous 4 months. On 12 May 2012, he visited a nearby general internal medicine clinic for the evaluation of left lower quadrant abdominal pain. He was referred to the Department of Internal Medicine at Asahi General Hospital (Asahi, Japan) for investigation and treatment. A bone marrow biopsy was performed on the same day. He was diagnosed as having myelopoietic disease. On 13 June 2012, he began taking oral hydroxyurea (Hydrea; Bristol-Myers Squibb, Princeton, NJ, USA).
His medical history revealed nothing significant. On 7 June 2012, he was unable to stop the gingival bleeding that had been ongoing for 5 hours. He then visited the emergency department of Asahi General Hospital and was referred to the Department of Dentistry and Oral Surgery.
At the initial visit, his chief complaints were bleeding from the gums and difficulty opening his mouth. The right molar teeth (47 and 48) showed Grade III mobility, and their gingivae were painful with continuous bleeding. His maximum mouth opening was 18 mm (Fig. 1A). The right molar teeth (46 and 47) showed Class III alveolar ridge deficiency on panoramic radiographs and were mobile teeth (Fig. 2A). We cauterized the bleeding points with an electrosurgical knife. We packed an absorbable haemostat (Surgicel; Ethicon, Somerville, NJ, USA) into the gingivae and sutured 3–0 silk threads above it. Finally, we used surgical dressing packs (COE-PAK; G.C. America, Alsip, IL, USA).
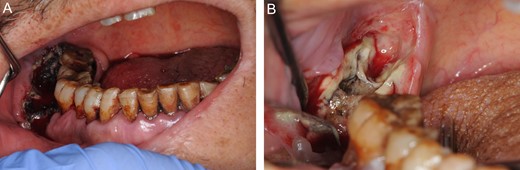
(A) The oral photograph at the initial visit, immediately after the gauze with the astringent has been removed. The maximum mouth opening is 18 mm. His gingivae are red and bloated. (B) The oral photograph after the extraction of teeth 47 and 48.

(A) Panoramic radiograph on 12 June 2012. (B) Coronal view of the computed tomography images on 25 June 2012. (C) Sagittal view of the computed tomography images on 25 June 2012.
The Internal Medicine Department assigned a clinical diagnosis of CMMoL, based on the blood and bone marrow examinations conducted on 13 June 2012. Computed tomography on June 25 indicated that bone absorption had nearly reached the right inferior alveolar canal, and a ring of sequestrum was present under tooth 47 (Fig. 2B and C). We diagnosed right mandibular osteomyelitis, based on these clinical features.
On 11 July 2012, the patient was hospitalized in the Department of Haematology ward because of significant anaemia and decreased platelet numbers. On the same day, the internal medicine specialist placed him on intravenous piperacillin–tazobactam (Zosyn; Pfizer, New York, NY, USA). He afterwards complained of severe pain in the socket (47 and 48), despite receiving the potent opioid analgesic dihydrohydroxycodeinone (Fentanyl; Daiichi-Sankyo, Chiyoda-ku, Tokyo, Japan). He also had limited mouth opening (18 mm). Hence, we decided to apply a surgical anti-inflammatory treatment in consideration of an acute blastic crisis. A bone marrow examination on July 13 showed no signs of acute blastic crisis of his CMMoL. After we consulted an internal medicine specialist, we planned a surgical procedure to clean the inflamed region in his mouth.
On the day before the surgery, he was administered a transfusion of platelet concentrate (20 units) and piperacillin–tazobactam to prevent bleeding and further infection. On July 20, with the patient under local anaesthesia, we surgically resected the right lower sequestrum and extracted molar 37, which displayed severe caries. The blood examination indicated improvement in the platelet count after the transfusion. After performing an inferior alveolar block, we removed the necrotic bone with ultrasonic bone surgery (Variosurg; NSK, Ashikaga, Tochigi, Japan) until there was bleeding from the bone surface (Fig. 3A and B). We placed gauze with tetracycline ointment in the socket and sutured 3–0 silk thread to compress it (Fig. 3C and D). We then placed a new haemostatic splint. The patient's pain disappeared on postoperative Day 3. On postoperative Day 7, his maximum mouth opening had increased to 28 mm. His maximum mouth opening ultimately reached 36 mm.
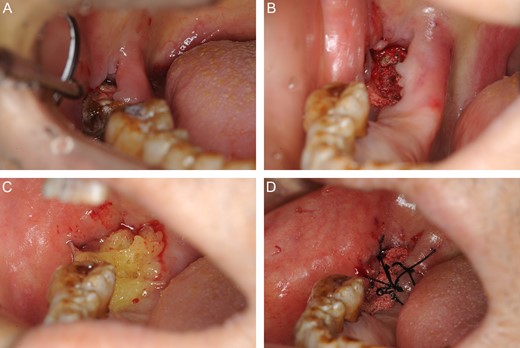
Photographs of the operative procedure. (A) Before surgery. (B) We removed necrotic bone with ultrasonic bone surgery until there was bleeding from the bone surface. (C) We placed gauze with tetracycline ointment in the socket. (D) We used 3–0 silk thread sutures to compress the gauze.
On August 11, his physical condition had sufficiently improved that he was discharged from the hospital. The formation of granulation tissue had nearly covered the surface of the bone, and all oral discomfort had disappeared (Fig. 4A). We later placed a bridge in the upper anterior teeth and added a partial denture (Fig. 4B). His occlusion was reconstructed, which contributed to a better quality of life.
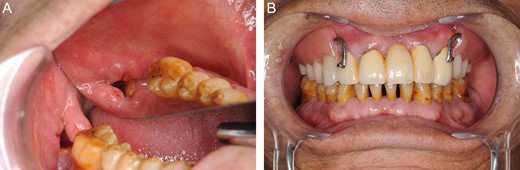
(A) Oral photograph on 18 October 2012. Formation of granulation tissue nearly covers the surface of the bone. (B) The oral photograph on 18 October 2012. We placed a bridge for upper anterior teeth 12, 11, 22 and 23, and a partial denture.
On 3 January 2013, he admitted himself to the hospital in the haematology ward because of exertional dyspnoea. The effects of transfusion had been poor since January 7. Splenomegaly and enlarged abdominal lymph nodes were verified by abdominal ultrasonography. The internal medicine specialists diagnosed CMMoL that was undergoing acute leukaemic transformation by bone marrow examination. He died on 10 February 2013 because of cardiac arrest, following haemorrhagic shock and cardiovascular failure due to CMMoL. He did not complain of pain around the right mandibular bone before his death.
Discussion
In all patients with CMMoL, every effort must be made to use the least invasive procedure possible. In the present patient, our deepest concerns were to have a proper balance between invasiveness and healing, and to avoid evoking an acute blastic crisis [9, 10]. Our most important goal was to alleviate the patient's discomfort by using a minimally invasive procedure to eliminate infection.
Based on haematology results, the oral surgery did not trigger the acute blastic crisis of CMMoL in this patient. After the surgery, he never complained of pain in the oral treatment region. The surgery was necessary to improve his oral environment and to prevent further infection and more pain. Because CMMoL is associated with a risk of acute blastic crisis and a poor prognosis, any surgical procedure in these patients must be considered on a case-by-case basis.
Conflict of Interest Statement
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}