





Abstract
Blunt traumatic infrarenal aortic injuries are unusual, and the formation of a delayed pseudoaneurysm of the aorta is even more rare. In this report, a young woman developed a small intimal flap of the infrarenal aorta after a motor vehicle accident which progressed into a 3 cm pseudoaneurysm after 3 months. Operative repair was successful and the patient recovered. This case illustrates the importance of repeat imaging of small blunt aortic injuries since progression can occur.
Introduction
Blunt traumatic infrarenal aortic injuries are rare, with a few case reports in the literature. A more common occurrence is an intimal flap which may form after blunt injury to the aorta, and most of these will resolve with anticoagulation alone [1, 2]. Blunt aortic injury which initially presents as an intimal flap (Grade I) may progress and evolve into an intramural hematoma (Grade II) or a pseudoaneurysm (Grade III). Aortic intimal flap progressing to dissection or pseudoaneurysm is an occurrence identified in 2% or less of the patients, and the majority of these occur in the thoracic aorta [1, 2]. This article presents the case of a young woman found to have an intimal flap in the infrarenal abdominal aorta after a car accident, and the injury progressed to a pseudoaneurysm over 3 months.
Case Presentation
A 47-year-old woman with a history of hypertension and smoking was involved in a high-speed motor vehicle accident and presented to the emergency department with back pain. Computed tomographic (CT) scans were obtained of her abdomen and pelvis. On a single image from the abdominal scan, what appeared to be either an intimal flap or a small amount of contrast extravasation outside of the infrarenal aorta could be seen. Her care providers had differing opinions as to what was being seen on the image. Since the abnormality was only seen on a single image, the exact etiology could not be delineated (Fig. 1). The patient was observed in the hospital overnight, had minimal complaints the next day, and was discharged on aspirin.
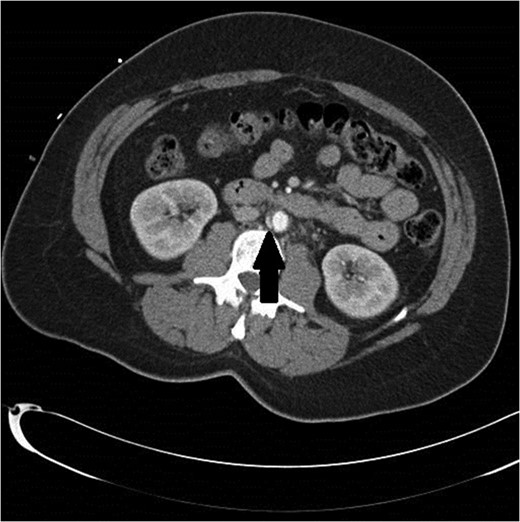
Initial CT scan shows enhancing vascular abnormality on the right side of the aorta, shown by the black arrow.
A follow-up CT scan was obtained 3 months later. At the location of the previous aortic abnormality, there was a 3 × 1 cm pseudoaneurysm that had formed and could now be clearly seen (Figs 2 and 3). The patient was asymptomatic.
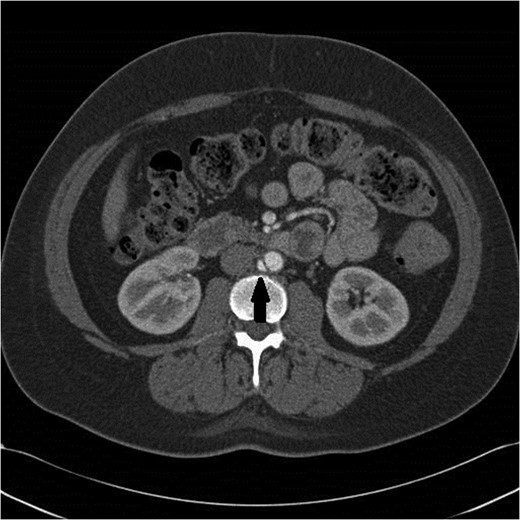
Pseudoaneurysm now clearly seen 3 months later.
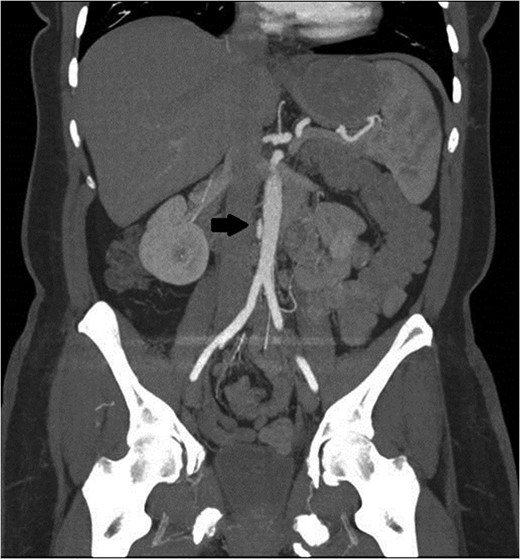
Black arrow pointing to pseudoaneurysm with enhancing flow outside of the aortic lumen.
Operative repair was recommended, but the patient’s aorta measured only 18 mm at the aortic bifurcation and was too small for even the smallest endovascular stent graft available at our institution. Therefore, an open replacement of her infrarenal aorta was performed using a Dacron 22 mm graft. In the operating room, a pseudoaneurysm was found on the posterior/lateral wall of the aorta. After the aorta was clamped and opened, a 4 mm tear in the intima had formed a mature channel into the pseudoaneurysm.
The patient recovered very well and was discharged from the hospital without complications. At her 2-year follow-up, she was in good health and had no further problems, but continues to smoke.
Discussion
Blunt abdominal aortic trauma occurs in only 0.04–0.1% of all nonpenetrating traumas [3, 4]. And the vast majority of these (92%) are associated with multiple other injuries [3, 5]. Our patient had no other injuries, and there was no retroperitoneal hematoma or other signs of vascular injury in the area, as is usually seen on CT when the aorta is injured [3–5]. The lack of other radiographic traumatic findings added to the initial confusion as to whether there was a true injury to the aorta, or if the single image was showing artifact or an enlarged vertebral vessel. Since the majority of intimal flaps heal with anticoagulation alone (55%) or remain stable (40%), a conservative plan including daily aspirin and re-imaging in 3 months was chosen [1].
When repeat imaging showed a 3 cm pseudoaneurysm, operative repair was necessary. This type of injury has been successfully repaired by endovascular techniques [4–7]. Endovascular repair was initially chosen for this case, but after measuring the patient’s aorta, femoral vessels and the degree of taper at the bifurcation, there was not an appropriate endovascular prosthesis available in such a small size. Thus, an open repair was performed by the author. Only one study has compared conventional open repair with endovascular repair for blunt injuries of the abdominal aorta and found similar results in both groups [8]. Endovascular repair is generally favored since the injuries tend to be focal and discrete, making them quite amenable to a short graft. Further, the patients usually have other significant injuries that would complicate a long, and potentially morbid, open operation on the aorta.
Although all blunt infrarenal aortic injuries are unusual, most of them consist of intimal flaps or dissections [3, 5–8]. A post-traumatic pseudoaneurysm, as this patient had, is even more unusual after blunt trauma. One prior publication did document the delayed occurrence of a post-traumatic infrarenal aortic pseudoaneurysm that was diagnosed 3 years after injury [9]. That patient was also treated by an open repair. Endovascular repair for pseudoaneurysms must include post-procedure angiography to document no evidence of a Type I or Type II endoleak, which could allow filling of the aneurysm sac and later rupture.
This case report highlights the need for delayed imaging for even minor intimal flaps or small aortic injuries after trauma, since progression does occur. While the vast majority of these injuries improve over time or remain stable, a small percentage will worsen and require intervention.
Conflict of Interest Statement
None declared.

{kind=link}
{kind=link}
{kind=link}