





Abstract
In cases of small bowel perforation with gross contamination, enterostomy has traditionally been the treatment of choice. An 86-year-old woman was diagnosed with perforative peritonitis. Emergency laparotomy revealed a small bowel perforation with gross contamination, and a T-tube enterostomy was performed. The T-tube was used for intestinal decompression for the first few days and was then accompanied by enteral feeding. When oral intake was sufficient, the T-tube was removed. The abdominal wall’s fistula healed within 2 days of removal. Except for wound infection, the patient developed no postoperative complications. Under specific circumstances, a T-tube enterostomy can be an effective alternative for a traditional enterostomy. Its advantages include less or no anastomotic leakage, easier management of fluid and electrolyte levels, postoperative enteral feeding from the tube, a shorter operative time and no need for a second operation to close the stoma.
Introduction
Perforation of the small intestine is not a particularly common entity; however, a pediatric case involving typhoid [1] and adult cases involving trauma [2] and iatrogenic perforations [3] have been reported in the literature.
In cases of perforative peritonitis, there are several treatment options. When contamination in the abdominal cavity is mild and localized, clinicians often prefer primary closure or resection with anastomosis; however, when contamination is severe and the intestine is damaged, enterostomy is often preferred.
Here, we present a case of perforation of the small intestine with gross contamination successfully treated with T-tube enterostomy.
Case Report
An 86-year-old woman who had undergone appendiceal cancer surgery before 2 years presented to our institution with acute onset abdominal pain lasting for several hours with no related episode of abdominal trauma. Physical examination showed tenderness in the lower left quadrant. Abdominal computed tomography showed free peritoneal air and fluid in the broad area of the abdominal cavity. The scan also showed that the bowel was diffusely dilated and had an edematous wall, and many diverticula along the descending and sigmoid colon.
Emergency laparotomy revealed gross contamination and dirty ascites, including intestinal contents spread over the entire abdominal cavity. The entire small intestine was edematous, and adhesions were extensive. A 7-mm perforation was visible on the small intestine (Fig. 1a), apparently a result of increased intraluminal pressure from a bowel obstruction. Intestine-to-intestine or intestine-to-abdominal wall adhesions were corrected. However, primary closure or anastomosis should be avoided because of edema and damage to the intestine. Instead of constructing an enterostomy, a 7-mm rubber T-tube (Willy Rusch GmbH, Germany) was inserted into the lumina through the perforation, and the tube was secured at the entry hole (perforation) with several stitches around the perforation (Fig. 1b). The T-tube was brought out through the abdominal wall at an appropriate site to avoid kinking of the tube. The intestine was firmly sutured to the abdominal wall with several stitches to prevent leakage (Fig. 1c).
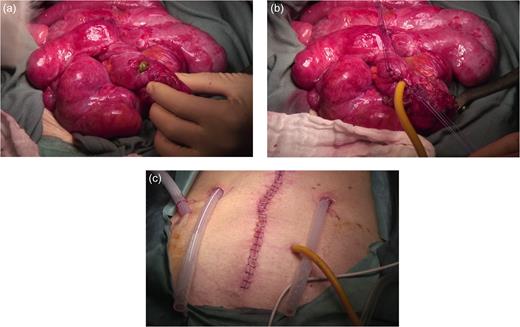
(a) Perforation on the edematous and damaged small intestine wall. (b) A rubber T-tube was inserted through the perforation and tightened in place with several stitches. (c) The T-tube was brought out through the abdominal wall, and the bowel was sutured to the abdominal wall at the exit site.
The patient remained in the ICU for 7 days due to sepsis caused by perforative peritonitis. She had a postoperative wound infection but experienced no other postoperative complications. The T-tube was kept open to decompress the intestine. On the 13th postoperative day, we used contrast medium to confirm that there was no dilatation or obstruction of the intestine, and no leakage into the abdominal cavity. We then started enteral nutrition through the T-tube. She required dysphagia rehabilitation after surgery and, although oral intake was initially insufficient, enteral nutrition through T-tube precluded any need for parenteral nutrition during the rehabilitation period.
By the 34th postoperative day, the patient’s oral intake was sufficient and her T-tube was removed. The fistula of the abdominal wall healed within 2 days (Fig. 2).

The fistula closed spontaneously within 2 days.
Discussion
In cases of small intestine perforation with gross contamination, an enterostomy is usually constructed, but several authors have reported the success of T-tubes, although predominately in small children. Rygl et al. [4] reported that they performed T-tube ileostomy in five cases of intestinal perforation in extremely low-birthweight neonates, and that all the patients survived without severe complications. Pandey et al. [1] also reported the usefulness of T-tubes in children with typhoid ileal perforation. To date, however, T-tube enterostomy for intestinal perforation in adult patients has not been reported.
There are several advantages to selecting T-tube enterostomy instead of traditional enterostomy. The patient may be able to avoid anastomotic leakage as a complication of primary closure or bowel resection with primary anastomosis, especially when extensive bowel damage exists, as in the case reported here. Second, since enterostomy output is usually liquid and high in volume, it can cause fluid and electrolyte imbalances. This can cause severe stress for the patients already in critical condition with sepsis caused by perforative peritonitis. Fluid replacement and antidiarrheal agents are often indicated for these patients. In contrast, the daily amount of discharge in our patient never exceeded 85 ml. A third advantage is that enteral feeding can be performed through the T-tube. Fourth, T-tube enterostomy takes less time than stoma construction. Finally, a T-tube can be easily removed from the body without anesthesia at bedside, and the fistula usually closes spontaneously [4]. Enterostomies require a further operation for closure under general anesthesia. Miller et al. [5] reported a colostomy closure-related morbidity rate of 20%.
A T-tube enterostomy can be an effective alternative to a standard enterostomy in selected cases; however, there are limitations. First, when the adhesion around the perforated intestine is too extensive to free the intestine from the surrounding organs, T-tube enterostomy should be avoided. A key component of this procedure is to tighten the T-tube at the entry hole and firmly fix the tube at the perforation site to the abdominal wall to prevent intestinal contents from leaking into the abdominal cavity. Second, although T-tube drainage for duodenal perforation [6] and esophageal perforation [7] has been reported, T-tube drainage would be insufficient in cases of colon perforation because of the solid content. Finally, when the perforation occurs near the terminal ileum, enteral feeding from the T-tube is largely useless.
In conclusion, in selected cases of perforation of the small intestine, T-tube enterostomy can be an effective treatment. The procedure’s advantages include no anastomotic leakage, easier management of fluid and electrolyte levels, postoperative enteral feeding from the tube, shorter operative time and no need for a second operation to close the stoma.
Conflict of interest statement
None declared.

{kind=link}
{kind=link}