





Abstract
Metastatic squamous cell carcinoma (SCC) from an unknown primary site to the colon has not been reported previously. A 75-year-old woman presented with a mass in the left submandibular region. Biopsy revealed a Class V lesion, but the histologic type was undetermined. Surgical resection of the left submandibular gland with cervical lymph node dissection was performed. However, SCC was seen in the lymph nodes only, with no tumor in the submandibular gland. Three months after surgery, computed tomography revealed that the preoperatively diagnosed lesion in the transverse colon had grown considerably. A laparoscopic right hemicolectomy was performed. Histological examination showed features of SCC, similar to the findings in the cervical lymph nodes. We report a rare case of synchronous metastatic SCC to the colon and cervical lymph nodes from a carcinoma of unknown primary site.
INTRODUCTION
Metastatic squamous cell carcinoma (SCC) of the colon is rare, but colonic metastases from primary tumors of the lung, esophagus and uterine cervix have been reported [1–4]. Carcinoma of unknown primary site is a well-recognized clinical disorder, accounting for 3–5% of all malignant epithelial tumors [1]. SCC is the most common histologic type of carcinoma of unknown primary site found in cervical lymph nodes [1,2,]. However, it is extremely rare for carcinoma of unknown primary site to metastasize to the gastrointestinal tract. We describe a case of synchronous metastatic SCC in the colon and cervical lymph nodes from a carcinoma of unknown primary site. Colonoscopy proved to be useful in diagnosing this condition.
CASE REPORT
A 75-year-old woman with a mass in the left submandibular region consulted the Department of Otorhinolaryngology. She required assistance in everyday life because of chronic rheumatoid arthritis and a previous cerebral hemorrhage. Fine-needle aspiration showed Class V cytology, but the exact histologic type was unclear. Left submandibular gland resection with cervical lymph node dissection was performed.
There was no evidence of tumor in the submandibular gland. Histological examination showed poorly differentiated SCC in the lymph nodes located at Level II (Fig. 1a). The patient was considered to have a carcinoma of unknown primary site because no primary lesions were found on detailed examinations of the esophagus, lung, uterine cervix and skin. A preoperative computed tomographic (CT) scan showed a small lesion with contrast effect in the transverse colon, which was difficult to distinguish from inflammation. Three months after operation, it was noted that the colonic lesion had grown considerably (Fig. 2). Fluorine-18 fluorodeoxyglucose positron emission tomography showed abnormal uptake in the transverse colon, but there was no accumulation at other sites (Fig. 3).
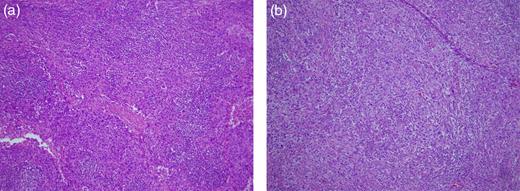
(a) Cervical lymph nodes. The specimen shows poorly differentiated SCC (H&E stain, ×40). (b) Metastatic colorectal tumor. The specimen shows poorly differentiated SCC similar to that seen in the cervical lymph nodes (H&E stain, ×40).
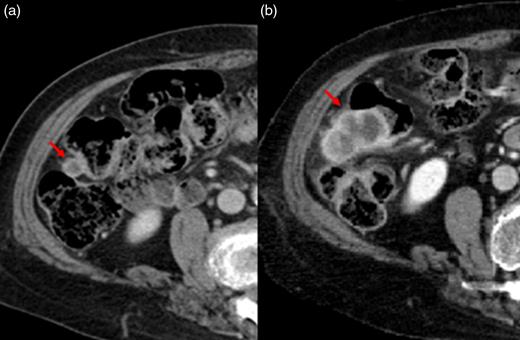
A preoperative CT scan showed a small lesion with contrast effect in the transverse colon, which was difficult to distinguish from inflammation (a). Three months after operation, it was noted that the colonic lesion had grown considerably (b).
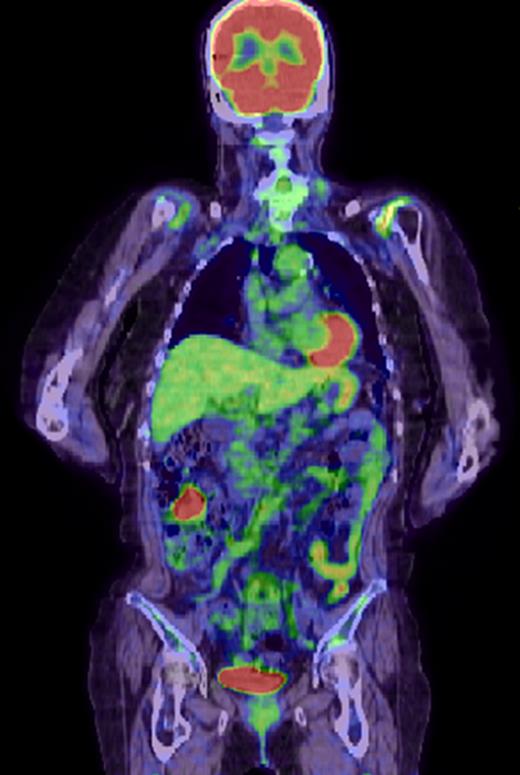
Fluorine-18 fluorodeoxyglucose positron emission tomographic scan shows positive findings in the transverse colon, with no other positive lesions.
Colonoscopy revealed a 40-mm submucosal tumor with an inflamed surface in the transverse colon. The appearance of this lesion suggested a metastatic lesion from another site, and biopsy was performed, but did not provide a definitive diagnosis (Fig. 4). Laparoscopic right hemicolectomy was then performed. Histological examination of the resected specimen showed features of poorly differentiated SCC, similar to that previously seen in the cervical lymph nodes (Fig. 1b). There were no elevations of serum tumor markers. The patient was discharged 11 days after surgery without any complications. No further adjuvant treatment was given because of her poor general condition.
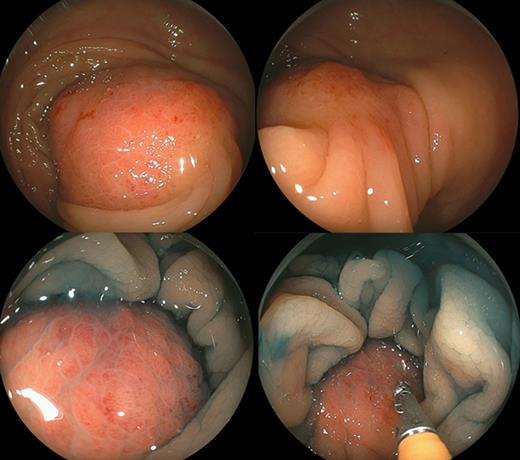
Colonoscopy reveals a 40-mm submucosal tumor with an inflamed surface in the transverse colon. Chromoendoscopy shows a tumor covered with normal mucosa. This lesion was a solid mass with a negative cushion sign (pressure applied to the tumor with a closed pair of biopsy forceps).
The lesion seen in the transverse colon on preoperative CT scans was in fact a small metastatic SCC. This report documents the clinical course of a patient with synchronous metastatic SCC to the colon and cervical lymph nodes from a carcinoma of unknown primary site. The patient remains free of disease after 1.5 years of follow-up.
DISCUSSION
This patient demonstrates two important clinical issues: (i) carcinoma of unknown primary site can present as colonic metastasis and (ii) colonoscopy is useful for establishing the diagnosis. First, carcinoma of unknown primary site can present with synchronous metastatic SCC to the colon and cervical lymph nodes. SCC from an unknown primary lesion with cervical lymph node involvement is found in ~5% of all head and neck cancers [5]. The most common clinical presentation is a painless, unilateral cervical mass. Level II lymph nodes are most frequently involved. Treatment of patients who have metastatic SCC with cervical lymph node involvement from a carcinoma of unknown primary site should be similar to that given to patients with locally advanced carcinoma. Radical neck dissection and radiotherapy with concurrent chemotherapy are recommended [5–7].
Visceral metastases from a carcinoma of unknown primary site are rare and generally have poor prognoses. The most commonly involved metastatic site is the liver, followed by lymph nodes, lungs, bones and brain. Gastrointestinal metastases are very rare. Squamous cell histology is a very rare subset of visceral metastases from carcinoma of unknown primary site. Recently, patients with carcinoma of unknown primary site have been divided into subsets with favorable (20%) and unfavorable (80%) prognoses. SCC involving the cervical lymph nodes is classified as belonging to the favorable subset, whereas colonic metastases belong to the unfavorable subset [6]. In our patient, synchronous metastatic SCC to the colon and cervical lymph nodes was completely resected. Postoperative adjuvant chemoradiotherapy was not given because the patient’s general condition was poor. As of 1.5 years after surgery, the patient is alive with no evidence of recurrence.
The second important clinical feature in our patient is that colonoscopy was useful for diagnosis. Metastases to the colon are relatively rare. Colonic lesions often represent direct invasion from adjacent organs or peritoneal dissemination, but lymphatic and hematogenous metastases from distant organs can also occur. A submucosal tumor in the gastrointestinal tract is one feature of lesions caused by lymphatic or hematogenous spread from other sites. Endoscopic examination in our patient revealed a gently elevated submucosal tumor with an inflamed surface. These findings are compatible with colonic metastasis from a carcinoma of unknown primary site.
Several reports have described colonic metastases from SCC [1–4]. Shimada et al. [3] reported a synchronous asymptomatic colonic metastasis from a primary esophageal SCC. Several reports have documented colonic metastases from the primary SCC of the lung [1,2]. Because endoscopic findings differ between epithelial tumor-like lesions and submucosal tumors, colonoscopy was consistently useful for establishing the diagnosis. A definitive diagnosis was possible after biopsy in some previously reported cases.
In conclusion, we reported a rare case of synchronous metastatic SCC to the colon and cervical lymph nodes in a patient with carcinoma of unknown primary site. Colonoscopy was useful for the diagnosis of this condition. Endoscopic findings were typical of metastatic submucosal lesions arising in the colon.
ACKNOWLEDGEMENTS
We are very grateful to our patient for providing her informed consent for publication of this case report. Patient anonymity is preserved.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}