





Abstract
Patients presenting with testicular pain and swelling mandate an urgent urology review and scrotal exploration to prevent testicle loss due to torsion. Other pathology masquerading as torsion is extremely rare but can occur. We present one such case. A 14-year-old male presented with a 1-day history of right testicular swelling and tenderness. He was apyrexial and denied any other symptoms. Blood tests demonstrated raised inflammatory markers. He had lower left-sided abdominal tenderness with a swollen, erythematous right hemiscrotum. During an urgent scrotal exploration for testicular torsion, a purulent hydrocele with a patent process vaginalis was noted, but no torsion. Post-operative abdominal pain mandated a general surgical review and subsequent appendicectomy. The patient made a full recovery. Acute suppurative appendicitis presenting as a urological emergency is extremely rare. To make a correct diagnosis and prevent multiple surgeries, a joint urological and general surgical assessment with a high index of suspicion is required.
INTRODUCTION
Both testicular torsion and appendicitis are common in childhood. The diagnosis of both is made on clinical grounds, and symptoms can be atypical. Surgical exploration is mandated for both. We present a case of appendicitis masquerading as testicular pathology.
CASE REPORT
A 14-year-old boy was referred by his GP to the paediatric emergency department with a 3-day history of intermittent lower abdominal pain and subsequently a 1-day history of right testicle tenderness and swelling. He had no bowel or urinary symptoms, no fevers or rigors, no history of trauma and denied any sexual activity. On examination, a slight tachycardia of 118 bpm was noted. There was some left-sided abdominal tenderness without rebound tenderness or guarding. The right hemiscrotum was mildly erythematous, oedematous and tender. The parents reported a retractile right testicle in infancy, which had not required surgical correction.
The patient was consented for scrotal exploration and taken to theatre with a clinical diagnosis of delayed presentation of testicular torsion. Surgery revealed a right-sided purulent hydrocele, a testicular appendage and patent processus vaginalis (PPV; Fig. 1 ). The hydrocele was evacuated and testicular appendage excised. The findings were attributed to acute torsion of the testicular appendage.
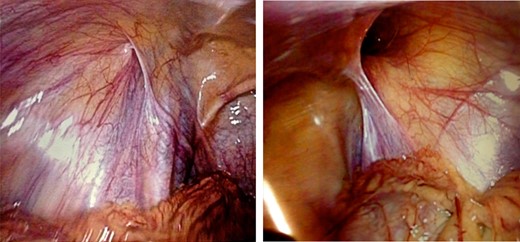
Closed left processus vaginalis and patent right processus vaginalis.
Post-operatively, the abdominal pains persisted and repeat examination noted focal right iliac fossa tenderness. Blood tests revealed a neutrophilia of 14.48 and a C-reactive protein of 54. On-call general surgical review led to a diagnostic laparoscopy, aspiration of turbid peritoneal fluid and the removal of an inflamed appendix. Histology confirmed severe acute transmural appendicitis. The patient made an uneventful recovery and was discharged on a course of antibiotics.
DISCUSSION
An acutely red, swollen and tender scrotum in a male adolescent should raise suspicion of testicular torsion and mandates prompt management. Testicular torsion occurs in 1 in 4000 males under the age of 25 years with a peak onset around 7–14 years of age [1]. With the exception of a high insertion of tunica vaginalis, very few risk factors for testicular torsion have been identified. Torsion usually occurs spontaneously and presents as acute onset testicular pain and swelling. Other causes of testicular swelling with or without pain include hernias, hydroceles, infection (epididymitis, epididymo-orchitis, mumps) and vascular malformations (e.g. varicocele). Ascites and congestive heart failure in adults also cause scrotal oedema [1]. Testicular pain due to intra-abdominal pathology tracking down a PPV is rarely recorded in the literature.
The processus vaginalis is an embryonic outpouching of the peritoneum present from the third month of gestation. It precedes the testis in its decent down the inguinal canal from the third month to the seventh month of gestation in males [2]. During the first year of life, the lumen fuses from the internal inguinal ring to the upper pole of the testes, leaving the most distal part to form the tunica vaginalis. Failure of the fusion leads to a PPV. The reported incidence in newborns is 70–80%, reducing to 30–40% by the age of 3–4 years and persisting to adulthood in 5.1% (autopsy assessment) [2]. It is twice as common on the right side. Failure of the fusion can present as a congenital inguinal hernia, a hydrocele or rarely due to intra-abdominal pathology such as appendicitis.
Appendicitis is extremely common with an incidence of 3–4 in every 1000 children. It can present at any age but usually presents after the age of 5 years [3]. Suppurative appendicitis is caused by luminal obstruction leading to abscess formation and necrosis of the appendix mucosa. It is more likely to have an atypical presentation with delays in seeking treatment. Furthermore, suppurative appendicitis presenting as testicular swelling and pain is an extremely unusual presentation. Abscess formation post appendectomy can lead to intra-abdominal collections, and tracking of these down a PPV causing testicular swelling has been described in the literature (Fig. 2). Appendicitis presenting as testicular swelling and pain with no history of intra-abdominal surgery is rarely reported [4].
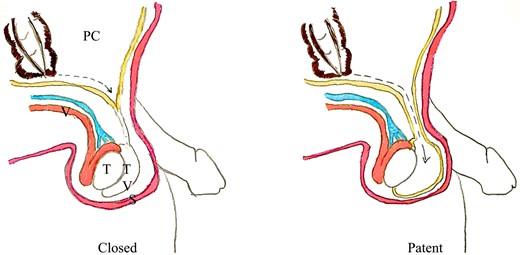
Tracking of pus down a closed and open processus vaginalis (PC, peritoneal cavity; V, vas deferens; T, testicle; TV, tunica vaginalis; S, scrotum).
Our case demonstrates the diagnostic difficulty faced by clinicians treating appendicitis with atypical presentation. The delay in diagnosis was caused by the clinically appropriate need to explore a patient presenting with an acute scrotum. The medical literature has suggested that patients can be safely observed and imaging utilized if a suppurative appendicitis is suspected, but an urgent scrotal exploration is required if testicular torsion is suspected, thus adding to the clinical dilemma [5, 6]. Furthermore, as in this case, anatomical variants such as testicular appendages can further confound a complex presentation. Alertness of the clinical team to deviation from normal post-operative recovery and re-examination led to an alternate differential diagnosis and appropriate referral and treatment in this case.
A PPV is extremely common in young males, and it decreases with age. Appendicitis and testicular torsion are common general surgical and urological emergencies. Appendicitis presenting as testicular pain is extremely rare (fewer than 10 cases in the literature) and remains a diagnostic challenge. Thorough history and examination, both pre- and post-operatively, are key to detecting atypical presentations of such conditions. Communication and inter-disciplinary team working remain key to avoid missed diagnoses in such complicated cases.
Written informed consent has been gained for the use of intraoperative images.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}