





Abstract
Simultaneous post-traumatic ipsilateral fracture of femur head and subcapital femur neck without hip dislocation is a rare presentation and easily missed on X-ray imaging. A 48 years old male, with a history of high-energy road traffic accident, presented to us with severe pain in the left hip region and inability to ambulate. Preliminary X-ray showed impacted subcapital fracture with varus angulation between femur head and neck. Further computed tomography (CT) scan imaging showed ipsilateral fracture of femur head and subcapital femur neck without hip dislocation. Primary total hip arthroplasty was performed. Presently patient is 5 years post-surgery and can ambulate without support. In conclusion, this fracture pattern, though rare, should be suspected in high-energy road traffic accident patients with shear forces acting at femur neck. It can best be diagnosed using 3D CT scan imaging. Primary total hip arthroplasty is an appropriate treatment in such patients.
INTRODUCTION
With speedy road transport, traumatic injuries to hip have varied patterns. One such rare fracture pattern is simultaneous post-traumatic ipsilateral fracture of femur head and subcapital femur neck without hip dislocation. It is easily missed on routine X-ray imaging. This injury pattern is clearly evident with 1–2 mm sections of 3D reconstructed computed tomography (CT) scan. Thus, acquaintance with this fracture pattern and clinical suspicion of its presence, especially in impacted subcapital fractures of femur neck, will prompt correct diagnosis and management.
Ipsilateral fractures of femur head and neck with dislocation of hip joint are more commonly encountered and are well described in the English literature [1–4]. Contrary to this, post-traumatic ipsilateral fracture of the femur head and subcapital femur neck without hip dislocation finds its mention in isolated case reports; two cases by Kang—II Kim et al. [5] and one case by Dieme et al. [6]. We describe a similar rare medley and highlight probable mechanism of development, best diagnostic investigation and its appropriate management.
CASE REPORT
A 48 years old male presented with history of road traffic accident. While driving at high speed, his bike collided with a truck traveling in opposite direction. Patient tried to avert fall using his left lower limb, but instead, was dragged along with the bike; his left lower limb caught in between the bike and road. Subsequently, he fell with his left hip caught between the floor and bike. He also suffered additional injuries to his head and chest.
Following trauma patient had left-sided chest pain, frontal headache and severe pain in his left hip region. After hemodynamic stabilization and preliminary treatment for his chest and head injuries, he was evaluated for left hip region pain. Clinically patient had left anterior hip joint line tenderness. Initial X-ray imaging showed impacted subcapital fracture of femur neck, with varus angulation between femur head and neck (Fig. 1), which prompted detailed radiological evaluation. A 3D reconstructed CT scan imaging disclosed a separate fracture line in femur head, with a detached inferior head fragment (Fig. 2); thus, the patient had concurrent ipsilateral fracture of femur head and neck without hip dislocation. We decided to treat this fracture pattern surgically with either osteosynthesis and fixation, or primary total hip arthroplasty. Via posterolateral approach to hip, femur head and neck fractures were exposed. Proximal femur fragment showed severe impaction of cancellous bone, making chances femur head salvage with osteosynthesis precarious. Thus, we performed primary uncemented total hip arthroplasty (Fig. 3). Presently, the patient is 5 years post-surgery without any complaints and ambulates without support or limp.

Antero-posterior radiograph showing subcapital fracture line of left femur neck.
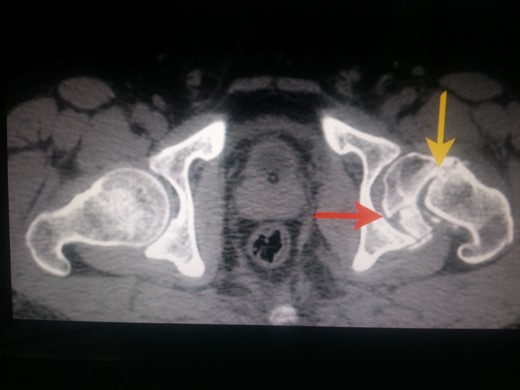
CT scan image of the patient in transverse cut. Yellow arrow pointing to the subcapital fracture line of left hip and red arrow pointing to the oblique fracture line of left femur head.
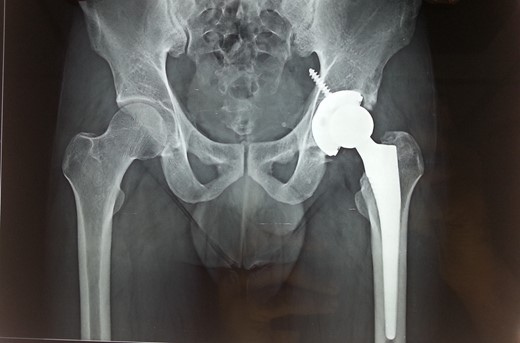
Recent 5 years follow-up antero-posterior radiograph image of the patient with uncemented total hip arthroplasty prosthesis in situ.
DISCUSSION
With a rising number of road traffic accidents, chances of trauma to hip increase, producing varied complex fracture patterns. One such facture pattern is post-traumatic ipsilateral fracture of the femur head and subcapital femur neck without hip dislocation. On extensive literature review, similar cases are reported in only two citations: first by Kang—II Kim et al. [5] and the other by Dieme et al. [6].
In our case, this fracture pattern developed due to shear forces acting on femur neck followed by lateral impaction. Shear forces developed as the patient's bike slid and fell after collision. In an effort to avert the fall with his left lower limb, weight of falling body and bike created a downward acting force, along the supporting lower limb, while ground reaction forces acted in an upward direction. Thus, with lower limb abducted at hip, knee locked in extension and opposing forces acting along limb, maximum shear forces acted on femur neck. When weight of the falling bike and patient's body exceeded ground reaction forces, subcapital fracture of femur neck developed.
With the continued momentum of the falling bike, patient's hip went into extension, adduction and external rotation, followed by lateral impaction, as the patient fell. Due to extension, adduction and external rotation along with lateral impaction, distal neck fragment, created by subcapital femur neck fracture, impacted against femur head fragment, creating an additional fracture of femur head and an inferior femur head fragment. Additional fracture line was located in inferior half of femur head, in sagittal plane. Thus, the patient finally developed ipsilateral fracture of femur head, with subcapital fracture of the femur neck, without hip dislocation.
Preliminary radiographs showed impacted subcapital fracture of femur neck with varus angulation between femur head and neck. Evidence of such complex fracture pattern on X-ray prompted further imaging to delineate fracture anatomy. The 3D reconstructed CT scan imaging showed the presence of additional fracture of femur head. Real-time viewing of the successive CT images on a dicom viewer best exemplified the fracture anatomy.
This fracture pattern is not included in the existing classification system of femur head fractures [7, 8]—Pipkin's classification [7]. We propose to modify Pipkin's classification to include this fracture pattern, by further dividing Pipkin's type III into IIIa and IIIb (Table 1).
Proposed modification of Pipkin's type III fracture
| Pipkin's type III fracture | |
| IIIa | Ipsilateral concomitant fracture of femur head and neck fracture without hip dislocation |
| IIIb | Ipsilateral concomitant fracture of femur head and neck fracture with hip dislocation |
This fracture pattern involves extensive damage to cancellous bone and vascularity of femur head. Osteosynthesis in such scenario demands prolonged immobilization. Such attempt is associated with high chances of avascular necrosis, subchondral collapse, secondary osteoarthritis and failure of fixation. The patient may have to undergo second surgery, total hip arthroplasty, to tide over. This second surgery demands special surgical expertise and will incur additional financial and emotional constraints. Contrary to this, primary total hip arthroplasty in this scenario promises better clinical and functional results, quicker functional rehabilitation and is more cost effective. Thus, total hip arthroplasty is the appropriate primary treatment option in such fracture patterns. Kang—II Kim et al. [5] also agree with the superiority of primary total hip arthroplasty in management of such fracture patterns.
So to conclude, ipsilateral fracture of femur head, with subcapital fracture of femur neck, without hip dislocation is uncommon. It is seen in patients of high-energy road traffic accidents, leading to shear forces at femur neck followed by impaction of the distal femur neck fragment on femur head. It can best be diagnosed using CT scan imaging. Primary total hip arthroplasty is the appropriate treatment option.
CONFLICT OF INTEREST STATEMENT
None declared.
REFERENCES

{kind=link}
{kind=link}
{kind=link}