Abstract
Pseudoaneurysm (PA) following vascular reconstruction is a complication of bypass surgery. Historically, the mainstay of treatment was an open repair; the surgical management consisted of resection of the initial graft with reimplantation of a new bypass either into the original arteriotomy or to a more distal target. Placement of a stent graft to exclude the PA is a viable option. We present a case of an 85-year-old man with prior history of polytetrafluoroethylene femoral–popliteal bypass now with an 8 × 5.6 cm PA of the distal anastomosis site treated with endovascular placement of a Viabahn stent.
INTRODUCTION
Pseudoaneurysm (PA) formation has been described in the literature as a delayed presentation in surgically revascularized patients. Given the rising number of reconstructive vascular procedures, the increase in anastomotic PA cases is expected [1]. Potential degeneration of biosynthetic grafts with aneurysm formation is a well-known problem with a reported incidence of up to 7% [2]. Implantation of a stent graft for treatment of a PA is a valuable treatment option in native arteries, as well as bypass grafts, as reported by Magnetti et al. [2]. In high-surgical-risk patients, the placement of a stent graft provides a safe and effective option for the treatment of anastomotic PA. We present a case of an 85-year-old man with prior history of polytetrafluoroethylene (PTFE) femoral–popliteal bypass now with an 8 × 5.6 cm PA of the distal anastomosis site treated with endovascular placement of a Viabahn stent. Of note, the patient underwent open thrombectomy and patch angioplasty of the site 10 years prior. Proper written consent was obtained from the patient prior to the creation of this case report.
CASE REPORT
An 85-year-old African-American male with a history of peripheral arterial disease (PAD) presents to our office with complaints of left leg pain and swelling. He has a past medical history of PAD, coronary artery disease, carotid stenosis, hypertension, prostate cancer, non-sustained ventricular tachycardia, COPD, recurrent gastrointestinal bleeding and end-stage renal disease dependent on hemodialysis. His prior surgeries include coronary artery bypass grafting, bilateral carotid endarterectomy, esophagogastroduodenoscopy with clipping, automatic implantable cardioverter-defibrillator placement and tunneled dialysis catheter placement. He also had a history of a femoral–femoral bypass with PTFE and subsequent left-sided femoral–popliteal bypass with PTFE. In 2005, he presented with acute limb ischemia of the left lower extremity (LLE) requiring open thrombectomy and endarterectomy of the distal anastomosis site of the femoral–popliteal bypass and repair with Vascu-Guard patch angioplasty. He now presents to our office with pain in the left posterior knee as well as below the knee swelling of the LLE. On physical exam, he had a large pulsatile mass of the posterior knee, the popliteal vessel had a palpable pulse and Doppler signals were present in the left posterior tibial and dorsalis pedis vessels; no motor or sensory deficits were present. Initial workup included an ultrasound (US) of the LLE to rule out a deep vein thrombosis and Duplex US for graft surveillance. Results of the imaging studies revealed left proximal graft stenosis >75% and a large arterial aneurysm in the medial mid left thigh at the site of pain, which appears to be at site of distal arterial graft. The decision was made to perform a CT angiography of the abdominal aorta with bilateral lower extremity runoff for further evaluation of the lower extremity anatomy and PA (Fig.
1). The results of the CT angiography showed a patent femoro–popliteal bypass graft and a PA, which measures 8 × 5.6 cm (Fig.
2) at the distal anastomosis compressing the popliteal artery (Fig.
3). Due the patient's multiple comorbidities and prior surgeries, the decision was made to repair the PA via an endovascular approach. The patient was taken to the vascular catheter laboratory and underwent LLE arteriogram with exclusion of the LLE PA with an 11 × 10 mm Viabahn stent. He underwent balloon angioplasty of the popliteal vessel and placement of a 6 × 80 mm Bard life stent. Completion arteriogram was performed and showed adequate runoff, pulse exam was comparable to preoperative examination with monophasic Doppler signals. The bypass entry site was closed via cut down and interrupted 5-0 Prolene suture. The PA was then aspirated with the Cook introducer needle; 20 cc of serous fluid and 60 cc of old non-pulsatile blood were aspirated. The operative site was closed in a layered fashion and the patient was maintained on a heparin drip as bridge to warfarin (Coumadin) and received a 300-mg clopidogrel (Plavix) bolus. Postoperatively, the heparin drip was continued until his international normalized ratio (INR) was therapeutic. On postoperative day (POD) 3, he was found to have a small hematoma at the femoral–femoral bypass access site, the heparin drip was held and a sandbag was applied to the area. On POD 4, his INR was therapeutic and the hematoma was non-expanding or pulsatile, the decision was made to discharge home.
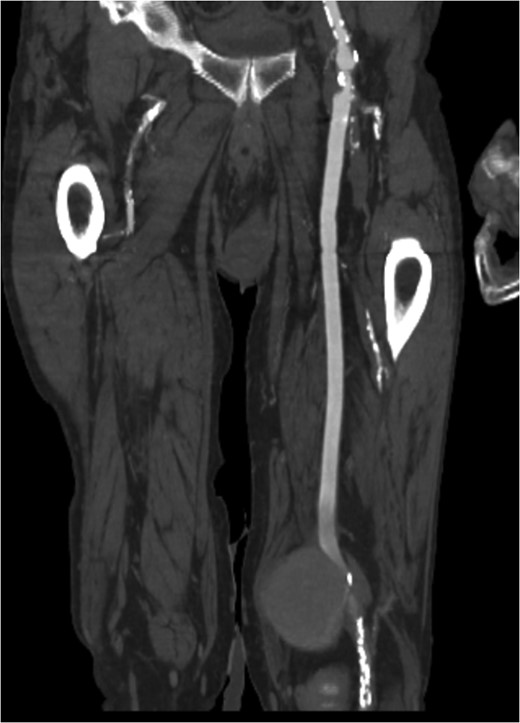
Figure 1:
Coronal view of popliteal PS of distal anastomosis site of femoral–popliteal bypass.
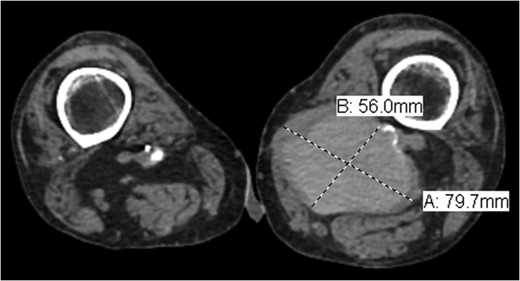
Figure 2:
Axial view of popliteal PS measuring 7.97 × 5.6 cm.
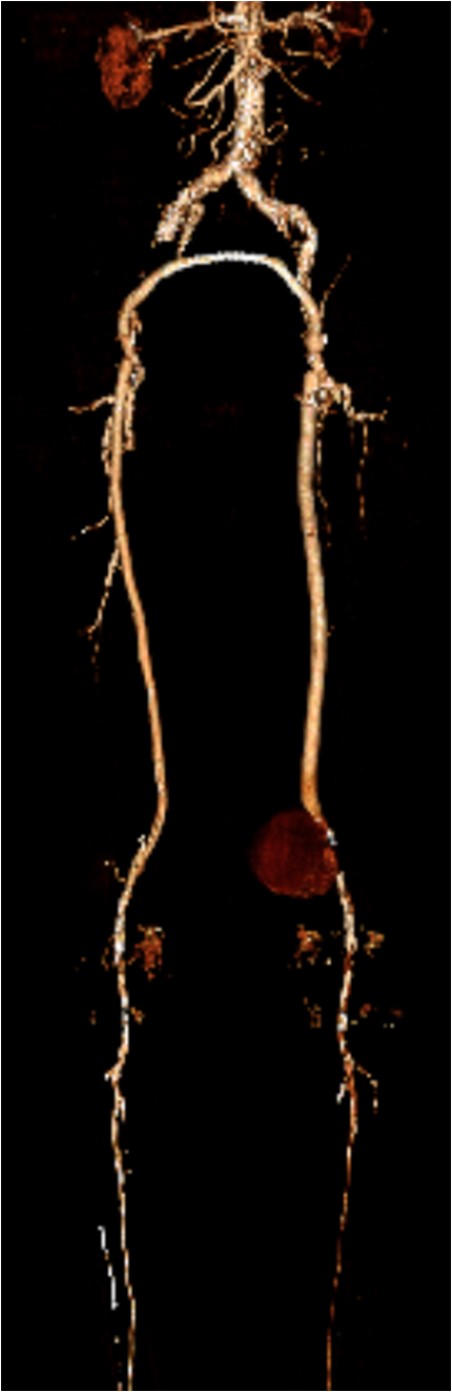
Figure 3:
Three-dimensional reconstruction image of PS.
DISCUSSION
PA, also known as a false aneurysm, is a result of an injury to the arterial wall that allows extravasation of blood, but is contained by the adventitia or surrounding perivascular soft tissue. Popliteal PA is usually a result of trauma or iatrogenic. The cumulative risk of a clinically significant PA after surgery is 2–6% [3]. There have been reports of popliteal PA following total knee arthroplasty, acupuncture and percutaneous transluminal angioplasty [4–6]. To the best of our knowledge, we present the first case of popliteal PA of the distal anastomosis of a femoral–popliteal bypass following patch angioplasty 10 years prior.
The clinical presentation of popliteal PA may vary from patient to patient. Our patient presented with compressive symptoms and unremitting pain. As reported by Marković et al. [1], compressive symptomatology compromises only 10% of presenting patients. Other presentations include acute and chronic limb ischemia, bleeding secondary to rupture and an asymptomatic pulsatile mass [1]. Although the majority of PA is secondary to trauma or iatrogenic injury, other etiologic factors are postoperative infection, suture fatigue, poor suture material, postoperative nicotine use, recurrent operations to the same site and mechanical obstruction [7]. If left untreated, PA may lead to thrombosis, rupture or distal embolization [8].
Indications to repair a PA include active hemorrhage, impending compartment syndrome and severe unremitting pain; as our patient had presented. The standard of care is early intervention with interposition graft placement as the treatment of choice. Although stenting of PA has been reported in the literature for over a decade, reports of endoluminal stent graft placement to treat false aneurysms of infra-inguinal bypass grafts are few [3]. Other non-operative techniques for the management of PA include US-guided compression, thrombin injection and coil embolization [9].
Popliteal PA following revascularization is a rare occurrence and may present many years later. They range in their presentation from asymptomatic pulsatile mass to acute rupture with hemorrhage. The identification and resolution of these lesions are aided by advanced imaging techniques, proper operative planning and patient-specific treatment options. In patients with multiple comorbidities, deemed high risk for cardiac events during surgery, an endovascular approach is a safe and viable option. We describe the successful treatment of a large PA at the distal anastomosis of a femoral–popliteal bypass graft using an 11 × 10 mm Viabahn stent with subsequent aspiration of the PA.
Conflict of interest statement
None declared.
REFERENCES
1Marković
DM
, Davidović
LB
, Kostić
DM
, Maksimović
ZV
, Cinara
IS
, Cvetković
SD
, et al. .
Anastomotic pseudoaneurysms
.
Srp Arh Celok Lek
2006
;
134
:
114
–
21
.
2Magnetti
F
, Thalhammer
C
, Hechelhammer
L
, Husmann
M
, Pfammatter
T
, Amann-Vesti
B
.
Spontaneous pseudoaneurysm of a femoro-popliteal Omniflow II graft treated with a stentgraft
.
Vasa.
2010
;
39
:
196
–
8
.
doi:10.1024/0301-1526/a000028.
3Rajachandran
M
, Klym
K
, Salvaji
M
.
A quick fix: graft rescue for iatrogenic pseudoaneurysm
.
J Invasive Cardiol
2007
;
19
:
E19
–
22
.
4Agarwala
S
, Mohrir
G
, Dotivala
S
.
Posttraumatic pseudoaneurysm of popliteal artery following total knee arthroplasty
.
Indian J Orthop
2013
;
47
:
101
–
3
.
5Kao
CL
, Chang
JP
.
Pseudoaneurysm of the popliteal artery: a rare sequela of acupuncture
.
Tex Heart Inst J
2002
;
29
:
126
–
9
.
6Derom
A.
Ruptured pseudo-aneurysm of the popliteal artery after percutaneous transluminal angioplasty
.
Acta Chir Belg
2003
;
103
:
102
–
4
.
7Hollier
L
, Batson
R
, Cohn
I
.
Femoral anastamotic aneurysms
.
Ann Surg.
1980
;
191
:
715
–
20
.
8Melissano
G
, Di Mario
C
, Tshomba
Y
, Civilini
E
, Gimelli
G
, Nicoletti
R
, et al. .
Endovascular treatment of a noninfected anastomotic juxtarenal aortic aneurysm
.
Tex Heart Inst J
2000
;
27
:
408
–
11
.
9Rundback
J
, Haug
J
, Herman
K
, Manno
J
, Cerda
M
.
Percutaneous stent-graft repair of anastomotic pseudoaneurysms following vascular bypass procedures: a report of two cases
.
Case Rep Vasc Med
2013
;
2013
:
124832
.
Published by Oxford University Press and JSCR Publishing Ltd. All rights reserved. ©
The Author 2016. This is an Open Access article distributed under the terms of the Creative Commons Attribution Non-Commercial License (
http://creativecommons.org/licenses/by-nc/4.0/), which permits non-commercial re-use, distribution, and reproduction in any medium, provided the original work is properly cited. For commercial re-use, please contact journals.permissions@oup.com







{kind=link}