





Abstract
Penile metastases are rare in colorectal cancer. We report the first case of such a recurrence in a patient who had undergone an extralevator abdominoperineal resection with vertical rectus abdominis myocutaneous flap perineal reconstruction. The patient was treated with curative intent by total penectomy.
INTRODUCTION
Although a richly vascularized organ with important circulatory communications, the penis is seldom the site of metastases. Since Eberth first reported it in 1870 there have been approximately 300 cases in the English language literature [1]. The primary tumour sites are principally the genitourinary organs, mainly the bladder and prostate gland. Only in 15.7% is the primary from the colon. Metastatic disease isolated to the penis and amenable to potentially curative treatment is very uncommon [1–3]. This is the first case of isolated penile metastasis following abdominoperineal resection (APER) with perineal vertical rectus abdominis myocutaneous (VRAM) flap reconstruction.
CASE REPORT
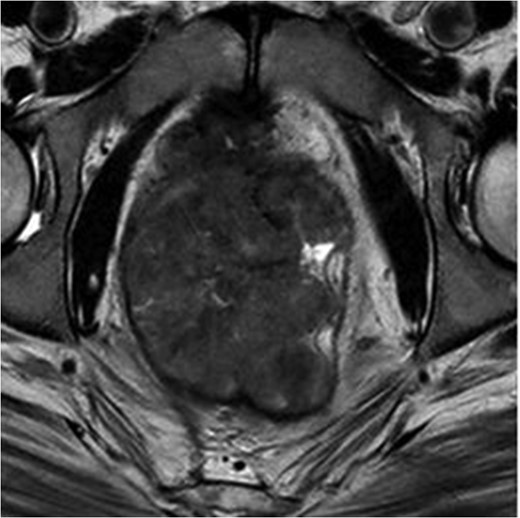
MRI pelvis. T2 waited axial image through lower pelvis through the large polypoid rectal tumour with T3 extension involving the CRM.
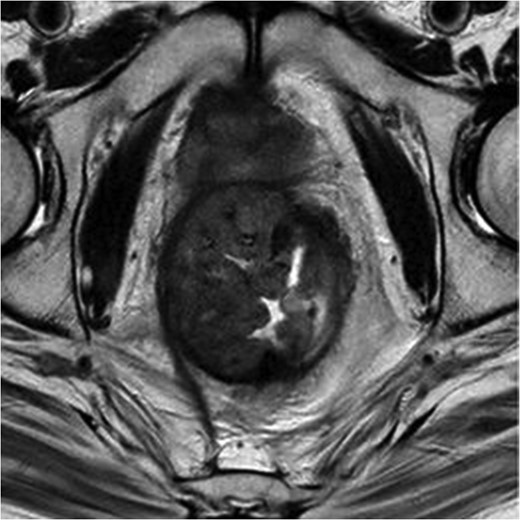
MRI pelvis. T2 axial image through pelvis demonstrating limited response to chemoradiotherapy with tumoral margins still predicted positive.
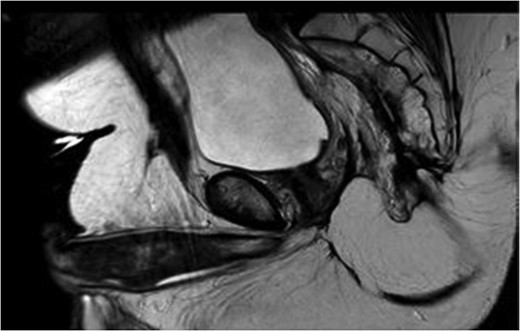
MRI pelvis large field T2 sagittal image through penile shaft showing the lesion involving the corpora cavernosum with extension in the spongiosum.
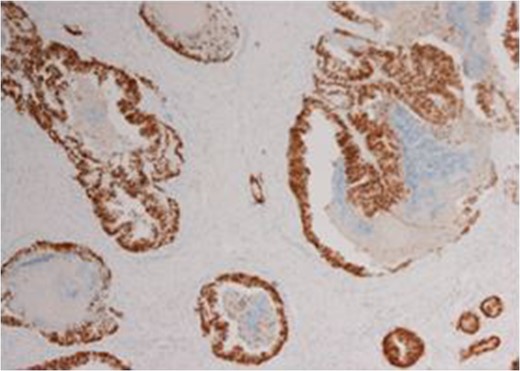
Immunohistochemistry of the biopsied lesion demonstrating CDX2 positivity.
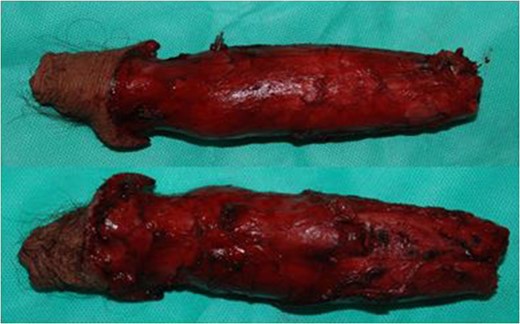
Dorsal and ventral view of specimen following total penectomy.
DISCUSSION
It is still a controversial subject the reason why the penis, despite its vascularization is a rare site for metastasis. It has been postulated that the route of metastasis include retrograde venous or lymphatic spread, local direct extension, arterial embolism or instrumental spread [1, 2, 4]. Currently the most accepted theory is the mechanism that involves retrograde venous spread from pudendal to the dorsal venous system of the penis [2, 4]. The most common type of presentation is malignant priapism followed by urinary retention, penile nodules, ulceration, perineal pain, oedema, infiltrative enlargement, dysuria and haematuria, with the corpora cavernosa being the most common site of metastasis and the glans and corpus spongiosum infrequently involved [1]. Our case respected the above mentioned cavernosal involvement but also had mild extension into the corpus spongiosum, more to the fact that this isolated metastatic penile neoplasm is extremely rare.
Management of penile metastasis is mainly palliative [5] as this is a sign of poor prognosis and tends to be part of widely disseminated disease. The majority die within a year [6]. This however is not the case in our present communication.
Treatment plan is influenced by the size of the primary, extent of the metastatic spread, performance status of patient and also prognostic characteristics of the primary tumour [2, 5]. Treatment modalities include the combination of radiotherapy with chemotherapy, local excision and penectomy [2, 4]. In isolated disease, as described in this case, penectomy may offer the possibility of cure although such cases are very rare.
In conclusion, this is a case report of penile metastasis following rectal adenocarcinoma, being the first one described in a patient that had APER with VRAM flap reconstruction. The patient underwent complete penile resection for curative purpose contrary to palliative treatment. This report highlights the rarity of the penis as site of metastasis and marker of disseminated disease, however this is not the case in our report and albeit rare, cure can be achieved in isolated cases.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}