





Abstract
A 58-year-old man presented with paralysis and pain in the left leg, and a mass was found in his thigh. Because of the growth of the mass and the worsening of his symptoms, the patient visited our hospital. Multidetector computed tomography revealed a large deep femoral arterial (DFA) aneurysm. Surgical intervention was planned because of the large size of the aneurysm, the high risk of perforation and the worsening symptoms. Aneurysmectomy and revascularization of the distal DFA with an artificial blood vessel graft were performed. DFA aneurysms are extremely rare. These aneurysms have a high rate of rupture, and surgery plays an important role in their treatment. However, standard methods have not yet been established because of their rarity of DFA aneurysm. We describe a case of DFA aneurysm in a patient who was successfully treated with aneurysmectomy and revascularization with an artificial blood vessel graft.
INTRODUCTION
Peripheral arterial aneurysms are rare, and among these, deep femoral arterial (DFA) aneurysms are extremely rare [1–3]. DFA aneurysms are not associated with any characteristic symptoms, and their early diagnosis is difficult. These aneurysms have a high rate of rupture, and surgery plays an important role in their treatment. However, standard methods have not yet been established because of the rarity of DFA aneurysms [3–6]. We describe a case of DFA aneurysm in a patient who was successfully treated with aneurysmectomy and revascularization with an artificial blood vessel graft.
CASE REPORT
A 58-year-old man presented with paralysis and pain in the left leg, and a mass was found in his thigh. Because of the growth of the mass and the worsening of his symptoms, the patient visited a neighboring hospital. Computed tomography confirmed the presence of a femoral arterial aneurysm. He visited our hospital for more detailed examinations and medical treatment. Physical examination revealed a pulsatile mass with a diameter of 8 cm in the left thigh. The patient had no history of trauma, previous operations or interventions. He had medication-controlled hypertension. Multidetector computed tomography performed in our hospital revealed a large DFA aneurysm with an intraluminal thrombus (Fig. 1). An image diagnosis of a DFA aneurysm was made. There was no evidence of aneurysms or occlusive lesions in the other arteries. Surgical intervention was planned because of the large size of the aneurysm, the high risk of perforation and the worsening symptoms.
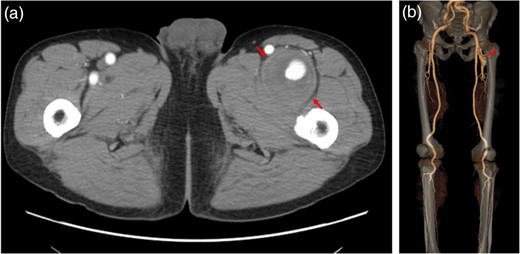
Multidetector computed tomography revealed a large DFA aneurysm (arrows show aneurysm).
The surgery was performed through a longitudinal groin incision. The sartorius muscle was preserved by splitting it along the muscle fibers. The DFA aneurysm was 5 × 10 cm in size. The proximal neck of the aneurysm was isolated 2 cm distal to the bifurcation. The deep femoral vein was found to be adhered firmly to the aneurysm. The common femoral artery, superficial femoral artery, superficial femoral vein and deep femoral vein were recognized and preserved (Fig. 2a). After clamping the DFA proximal and distal to the aneurysm, we opened the sac and found a massive thrombus. Aneurysmectomy and revascularization of the distal DFA with an artificial blood vessel graft were performed (Fig. 2b). The operation lasted for 416 min, and the operative bleeding was 690 ml. Pathological examination of the specimen revealed atherosclerosis in the vascular wall and confirmed that it was a true aneurysm.
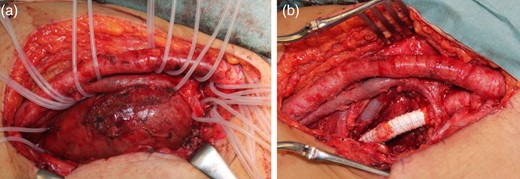
(a) The common femoral artery, superficial femoral artery, superficial femoral vein and deep femoral vein were recognized and preserved. (b) Aneurysmectomy and revascularization of the distal DFA with an artificial blood vessel graft were performed.
Following surgery, the patient's symptoms improved gradually. A follow-up multidetector computed tomography scan showed good blood flow in the graft, superficial femoral artery and popliteal artery (Fig. 3). The patient had an uneventful postoperative recovery and was discharged without complications.
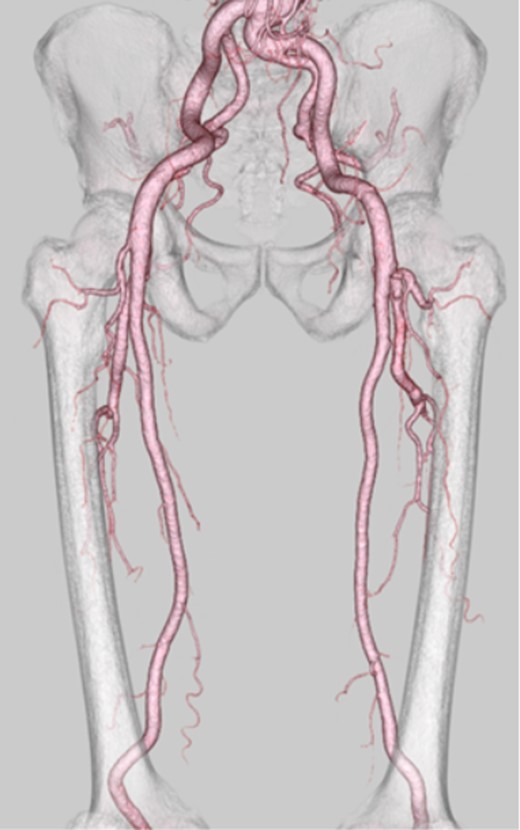
A follow-up multidetector computed tomography scan showed good blood flow in the graft, superficial femoral artery and popliteal artery.
DISCUSSION
DFA aneurysms are a rare form of peripheral arterial aneurysms [1–3]. Although many DFA aneurysms have been associated with other peripheral aneurysms or peripheral occlusive diseases, there was no evidence of aneurysms or occlusive lesions in the other arteries of our patient [4, 7, 8]. Therefore, we consider our case of an isolated DFA aneurysm to be extremely rare.
There are no characteristic symptoms of DFA aneurysms in the early stage, and their diagnosis is difficult. They are often found accidentally or after their enlargement, when symptoms include pulsating groin swelling, paralysis or pain in the leg, which were the symptoms that our patient experienced. Enlarged DFA aneurysms must be treated because of the high risk of rupture, which may cause severe complications, including hemorrhagic shock, ischemia of the foot, thigh embolization, thrombophlebitis and sciatic or femoral neuropraxia [1, 5, 9, 10].
Surgery plays an important part in the treatment of DFA aneurysms. Several treatment options, including simple ligation, revascularization of the distal DFA and bypass grafting to the popliteal artery, exist for DFA aneurysms; however, standard methods have not been established because of the rarity of DFA aneurysms. In our case, we performed an aneurysmectomy and revascularization to the distal DFA with an artificial blood vessel as the graft. Revascularization was performed to avoid thigh ischemia and preserve the collateral circulation if ipsilateral peripheral occlusive disease occurred. We believe that revascularization to the distal DFA should be done whenever it is technically feasible. In previous reports, the saphenous vein was successfully used as the graft. In the future, if the patient must undergo operations such as coronary artery bypass grafting or other peripheral arterial bypass grafting, the saphenous veins will be required for those surgeries. Therefore, we did not use the saphenous vein as the graft. In this case, we consider the surgery a success because the patient recovered well from the surgery without complications, his symptoms improved and the blood flow in the leg was preserved.
In conclusion, DFA aneurysms are extremely rare. Surgery plays an important part in the treatment of this disease, but standard methods have not been established because of its rarity. In our patient, we successfully performed an aneurysmectomy and revascularization to the distal DFA with an artificial blood vessel graft.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}