





Abstract
A 79 years old woman presented in a peripheral hospital with dyspnea, right-sided pleuritic chest pain and cough for 3 days. On examination, she was tachycardiac and tachypneic. She had reduced air entry bilaterally on auscultation. Computed tomography-pulmonary angiogram, performed in peripheral Hospital, confirmed the diagnosis of pulmonary embolism, and she was commenced on warfarin. Ultrasonography showed no evidence of deep venous thrombosis in legs; however, ultrasound of the abdomen revealed an aortic aneurysm. She was hemodynamically stable on transfer to vascular surgery department, and her complete clinical examination revealed a pulsatile mass in the central abdomen. Computed tomography angiogram of aorta showed 8.7-cm abdominal aortic aneurysm. Venogram performed during inferior vena cava (IVC) filter insertion showed that IVC was displaced and compressed due to this large aortic aneurysm, causing thromboembolism. An open repair of the aneurysm was performed with uneventful recovery.
INTRODUCTION
Pulmonary embolism is generally associated with risk factors grouped as stasis, venous injury and hypercoagulability. We report a case where a patient developed pulmonary embolism (PE) due to venous stasis caused by an unusual cause, i.e. a large abdominal aortic aneurysm (AAA) compressing and displacing the inferior vena cava (IVC). The relationship between the two was confirmed with a venogram during IVC filter insertion. This case also reminds an important clinical lesson of performing a complete clinical examination of patients including the abdomen, regardless of the absence of relevant symptoms.
CASE REPORT
A 79 years old woman was admitted in a peripheral hospital with symptoms of shortness of breath and right-sided pleuritic chest pain for 3 days. She had some cough but no hemoptysis. She had a past medical history of hypertension and was on amlodipine and indapamide. She was fully oriented in time and place and was mobilizing independently. She had no risk factors for hypercoagulable state, such as immobilization, malignancy, recent surgery, drugs and thrombophilia.
On examination, she was tachycardiac with a heart rate of 110 beats per minute. She had a normal blood pressure of 125/85 mmHg and was afebrile. Her respiratory rate was 22 breaths per minute and oxygen saturation was 90% at room air on pulse oxymetry. On auscultation, she had reduced air entry bilaterally, and there were no added sounds. She had no signs of deep venous thrombosis (DVT) in her legs. She also had no signs of heart failure or vena caval obstruction.
She had a blood D-dimers level of 8.2 nmol/l. Her routine blood tests were normal. Computed tomography-pulmonary angiogram (CTPA) showed emboli in right and left main pulmonary arteries and in several of the lobar and segmental branches. It showed a triangular area of increased density at the periphery of right mid-zone representing an acute pulmonary infarct. She was commenced on warfarin.
There was no evidence of DVT in leg on ultrasonography. An ultrasound of the abdomen was performed in peripheral hospital to rule out any intra-abdominal source of the embolus. It revealed an incidental 9-cm AAA.
She was transferred to the department of vascular surgery in a tertiary-care center for further management of this large AAA.
On arrival at our hospital, she was hemodynamically stable, with all vital signs within the normal range. Abdominal examination revealed a pulsating mass in the center of the abdomen. A computed tomography (CT) angiogram of aorta was performed for further evaluation that showed ectatic aorta from arch to the diaphragm. There was an 8.7-cm infra-abdominal AAA with extension into both common iliac arteries. The aneurysm neck was tortuous with an acute angle making endovascular repair challenging (Figs 1–4).
Decision of open repair of AAA was made. After stopping warfarin and reversing its effect, insertion of IVC filter was performed before the surgery. The inferior venogram during this procedure showed that the IVC was displaced to the right with external compression secondary to this large aortic aneurysm (Fig. 5).
A diagnosis of large AAA causing PE was made as it was found to be displacing and compressing the IVC, and causing venous thromboembolism. During the open repair of aortoiliac aneurysm, findings of venogram were confirmed, as aneurysm was found to be compressing IVC (Fig. 6). A large plaque was removed from the aneurysmal sac. A bifurcation synthetic graft was placed for inlay reconstruction, and the abdomen was closed in layers. Her recovery period was uneventful. She was able to sit on the chair on Day 3 after surgery and was mobilizing well in a week time.
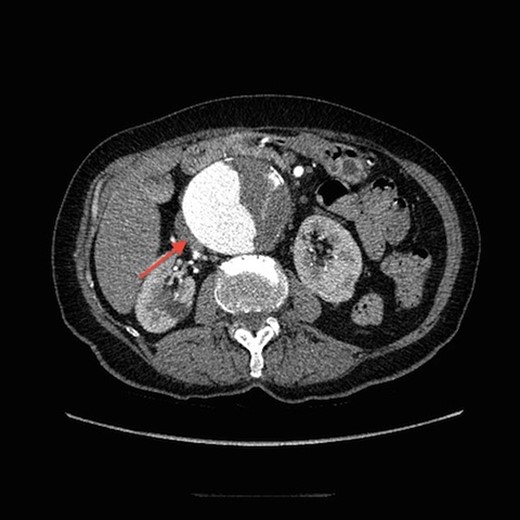
Transverse view of CT aortogram, showing compression of IVC (arrow).
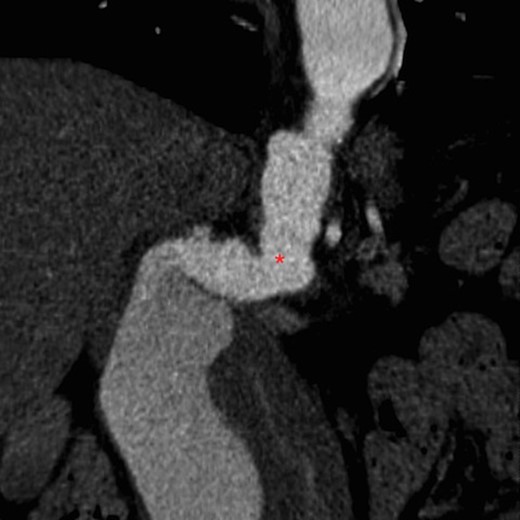
Tortuous angled neck of aorta on CT aortogram (asterisk).

Coronal view of CT aortogram showing compression of IVC (asterisk).
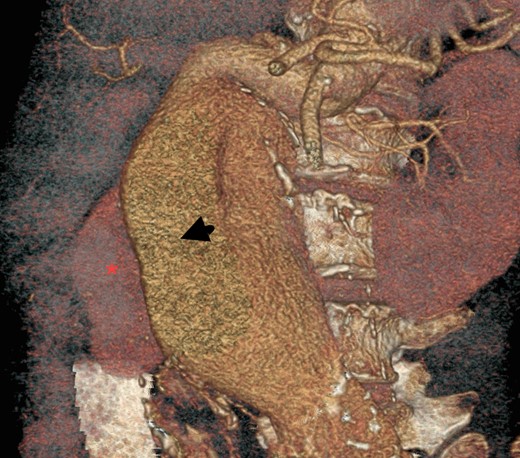
Three-dimensional construction of CT aortogram showing displaced and compressed IVC (asterisk) due to large AAA (arrow head).
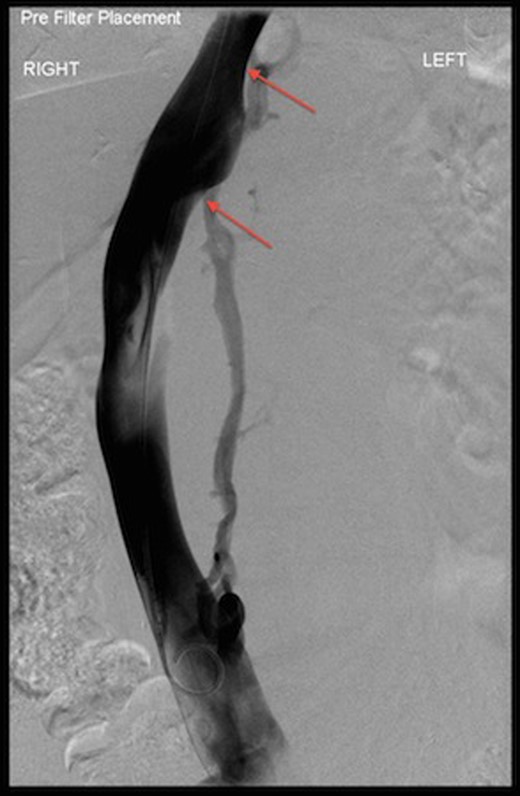
Venogram during IVC filter insertion showing indentation by AAA on IVC and its displacement (arrows).
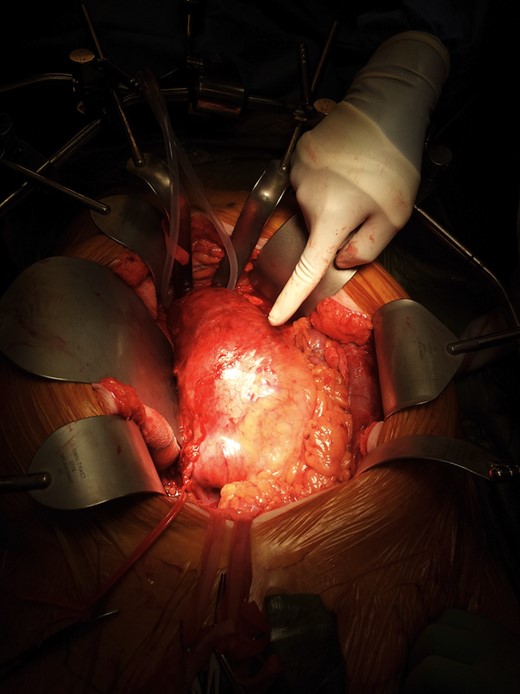
Intraoperative findings of large AAA.
DISCUSSION
Although PE can be idiopathic, it is mostly associated with risk factors described as Virchow's triad, comprising of stasis, vessel wall damage and hypercoagulability. Stasis results from changes in blood flow caused by factors, such as turbulence at bifurcations and irregular vessel lumen, e.g. atheroma or stenotic regions [1]. Other conditions causing stasis include immobilization, limb paralysis, heart failure, varicose veins and chronic venous insufficiency [2].
External compression of IVC can occur due to malignancy, ruptured AAA [3], traumatic hepatic hematoma [4] and polycystic kidneys [5]. In our case, a large un-ruptured AAA was found to be compressing and causing stasis in IVC, leading to PE.
Un-ruptured AAAs are usually asymptomatic but may cause symptoms from local compression, e.g. on the stomach, urinary tract and superior mesenteric artery [6]. Other symptoms include abdominal, back or groin pain and limb ischemia from embolism. The risk of rupture is dependent on the size of the AAA. In asymptomatic AAAs <5.5 cm, the risk of rupture is low, and therefore surveillance with periodic abdominal ultrasound is recommended [7]. In AAAs >5.5 cm, elective repair should be planned, as the risk of rupture is high [8]. CT scanning is generally used for operative planning to show the relationship of the aneurysm to the renal arteries as approach may change to thoracoabdominal if it extends above renal arteries. It also demonstrates involvement of iliac arteries.
Operative repair is either through open surgery or endovascular approach. Endovascular aneurysm repair (EVAR) is associated with less procedure-related mortality, short hospital stay and is unaffected by previous abdominal surgery. On the other hand, its follow-up with ultrasound and CT is lifelong. AAA-related re-interventions are more common after EVAR but typically are minor endovascular re-interventions, while laparotomy-related major re-interventions are more common after open repair [9].
Pulmonary embolism can be cryptogenic, but a thorough investigation should be carried out to find a cause. This must include a complete examination of the abdomen, pelvis and legs, regardless of patients being asymptomatic in these areas. Inferior vena cava venogram proves to be a useful tool to find a source of embolism, and to rule out external compression. Ultrasound of the abdomen remains a reliable tool for AAA screening. In AAA investigations, specific protocol imaging of IVC should be done to see any filling defect or external compression due to AAA. Early repair of large AAAs not only prevents the rupture but also relieves its local pressure effects.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}