





Abstract
Diverticulosis of the vermiform appendix is rare and usually asymptomatic or associated with mild, chronic or intermittent abdominal pain. A 52-year-old patient was admitted to our department due to lower abdominal pain. Assuming the second episode of diverticulitis of the sigmoid, a computed tomography (CT) was performed, and complicated sigmoid diverticulitis and an accentuated appendix without inflammatory signs were diagnosed. Laparoscopic sigmoid resection was performed with an intraoperative macroscopic inconspicuous appendix. Two months later, right-sided abdominal pain returned. CT scan showed increasing signs of thickened appendix. Because of a gallbladder polyp, a combined laparoscopic appendectomy and cholecystectomy with one additional laparoscopic access was performed. Pathology detected a small diverticulum of the appendix and a small tubular adenoma with low-grade intraepithelial neoplasia in the gallbladder. Although diverticulitis of the appendix is very rare, it should be considered in patients with right lower abdominal pain, and appendectomy should be performed even in macroscopic unsuspicious cases.
INTRODUCTION
Colonic diverticulosis of the sigmoid and descending part of the colon is common, but the right colon is rarely involved. The incidence of appendiceal diverticulitis in pathologic specimens is 0.2–1.5% [1]. Appendiceal diverticulosis was first described by Kelynack in 1893 [2] and is usually an incidental finding mostly without clinical symptoms. Sometimes, appendiceal diverticulosis can be associated with mild, chronic and intermittent abdominal pain over a period of a month or even years before diagnosis is made [3]. However, symptomatic appendiceal diverticulitis has a four times higher chance for perforation and a 30-fold increased mortality rate compared with simple appendicitis [4]. Diagnosis is often revealed by histopathological examination after appendectomy.
Diverticulosis of the vermiform appendix can be classified as congenital and acquired. The congenital ones involve all layers of the appendiceal wall and are very rare with only up to 50 reported cases in the world. The acquired form is more often caused by mucosal herniation through a muscular defect on the mesenteric border of the appendix. Clinical appearance of appendiceal diverticulitis differs to symptoms of classic appendicitis: clinical course of appendiceal diverticulitis is more often moderate and affects older male patients (>30 years of age) with a history of previous attacks.
Appendiceal diverticula are identified in 2% of appendectomies [5]. It is hypothesized that obstruction with subsequent inflammation predisposes to the formation of acquired diverticula. As described in the literature, appendiceal diverticulosis is not associated with colonic diverticulosis [3].
We report on a patient with inflammatory solitary diverticulum of the appendix covered by complicated sigmoid diverticulitis.
CASE REPORT
A 52-year-old man with a history of diffuse lower quadrant pain (left and right) presented to our outpatient department because of exacerbation of abdominal pain and fever. The pain was spasmodic and progressive in severity. The abdomen was soft with tenderness in deep palpation in the right and left middle and lower abdomen. Leukocyte count was 10 × 109/l, and CRP was elevated with 16 mg/dl.
Assuming a diverticulitis of the sigmoid, a computed tomography (CT) was indicated, demonstrating an acute complicated diverticulitis of sigmoid (IIb according to Hansen and Stock) [6]. The appendiceal region did not show signs of acute inflammation, but the appendix layer was slightly emphasized. After initiation of antibiotic treatment, an early elective laparoscopic resection of the sigmoid was performed [7]. Intraoperatively, the appendix was unsuspicious. A laparoscopic sigmoid resection with primary anastomosis was performed. Postoperative course was uneventful. The patient recovered well and could be released 6 days later.
Two months later, the patient was re-admitted to our outpatient department with more right-sided abdominal pain without peritonism. Signs for infection were not detectable by blood chemistry. Ultrasound of the abdomen showed no abnormalities except for a gallbladder polyp. A colposcopy did not reveal anastomotic problems. An outpatient management with symptomatic therapy was performed with slight improvement of the symptoms.
Three months later, the patient had exacerbation of the right lower quadrant pain. At this time, the pain was accompanied by fever and diarrhea appearing 4 days ago. Leukocyte count was still normal; CRP was slightly elevated (3.5 mg/dl). Repeated CT scan showed an increase in wall thickness of the vermiform appendix with mild surrounding reaction according to acute signs of inflammatory disease. A diagnostic laparoscopy with cholecystectomy and appendectomy was performed using standard four-port position for laparoscopic cholecystectomy [7] with only one additional incision (10-mm port) in the left lower quadrant for appendectomy. Intraoperatively, the appendix was suspicious and thickened. Pathologic analysis demonstrated one small appendiceal diverticula with inflammation (Fig. 1). The gallbladder showed a small tubular adenoma with low-grade dysplasia (Figs 2 and 3). The patient recovered well and was discharged 3 days later.
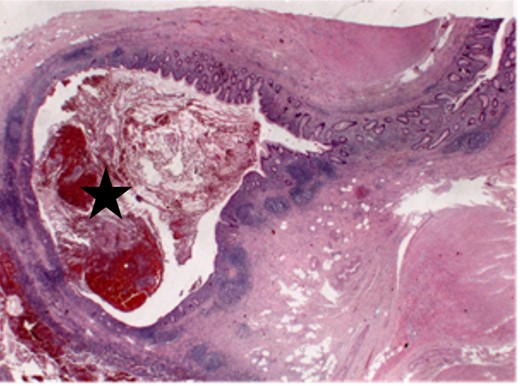
Small appendiceal diverticula with inflammation.
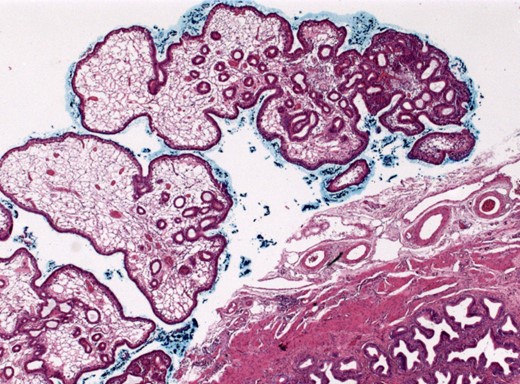
Overview of the gallbladder with tubular adenoma (25×, HE).
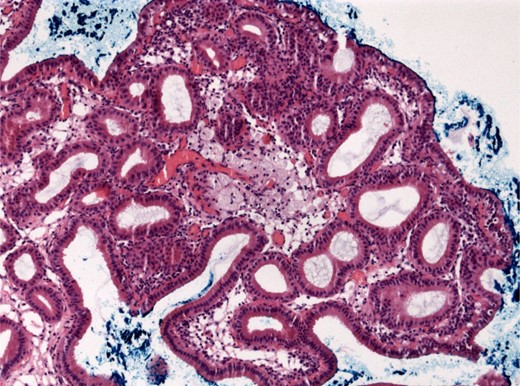
Gallbladder polyp in magnification (100×, HE).
DISCUSSION
In contrast to the sigmoid diverticulosis, diverticulosis of the appendix is rare. Appendiceal diverticulosis is usually asymptomatic; only in the case of inflammation, it causes right lower quadrant pain and can imitate an acute appendicitis. However, appendiceal diverticulitis manifests often after the third decade of life and accompanies with intermittent pain 1–14 days before diagnosing and has a history of previous attacks. As possible risk factors like chronic appendicitis, cystic fibrosis, age >30 years and male sex are discussed [8]. Appendiceal diverticulitis in symptomatic patients should be treated with early resection because of the risk for perforation with peritonitis [the rate of perforation of appendicitis with diverticulosis (27%) is higher than that of appendicitis alone (6.6%) [9]], massive gastrointestinal hemorrhage, abscess formation and for the potential role in the development of pseudomyxoma peritonei. In the case of an incidentally discovered appendix with diverticulosis, it should be removed because one-third of all patients with diverticulosis of the appendix experience an acute inflammation.
Almost all appendiceal diverticula are acquired. Commonly, they are multiple, but a solitary diverticulum can occur [5].
Appendiceal diverticula are proposed to discover by prolapse of the mucosa through the muscularis propria because of increased intraluminal pressure. Appendiceal diverticulosis may occur in the absence of colonic diverticulosis. This might be explained by the appearance of a small lumen with increased thickness of the submucosa and muscular wall, as well as atrophy of the mucosal lymphoid tissue caused by chronically elevated luminal pressure [3].
In our case, we observed an acute complicated diverticulitis of sigmoid and performed laparoscopic sigmoid resection. Macroscopically, the appendix was initially unremarkable. Only few months later, the patient developed again right lower quadrant pain, showing signs for acute and chronic appendicitis in radiologic imaging.
A second laparoscopic operation was necessary. Only one additional laparoscopic access was needed for cholecystectomy and appendectomy. Intraoperatively, the appendix was thickened and suspicious. Histology detected one small single diverticula of the appendix with inflammatory signs that could not be detected even intraoperative.
In conclusion, in the case of intermittent chronic right-sided lower abdominal pain and an emphasized appendix layer, resection of the appendix should be indicated even if the appendix is macroscopic unsuspicious.
CONFLICT OF INTEREST STATEMENT
None declared.
ACKNOWLEDGEMENTS
We thank Prof. Dr med. F. Fend and PD Dr med. P. Adam from the Department of Pathology and Pathological Anatomy for providing histological images and histopathological expert advice.

{kind=link}
{kind=link}
{kind=link}