





Abstract
Lumbar artery pseudoaneurysms are infrequent complications of penetrating trauma. When present, they are often accompanied by other injuries; however, we report the case of an isolated traumatic lumbar artery aneurysm resulting from a single knife stab. The lesion was successfully treated with endovascular microcoil embolization. While these injuries are uncommon, the surgeon must maintain a high index of suspicion, even with seemingly uncomplicated injuries, as a missed traumatic pseudoaneurysm may be life threatening.
INTRODUCTION
Arterial pseudoaneurysms are a well-documented occurrence in the setting of both penetrating and blunt traumatic injuries [1]. However, traumatic lumbar artery pseudoaneurysms (LAPAs) are less frequent, their documentation in the literature being limited to several case reports [2–5]. Traumatic LAPAs are often accompanied by serious concomitant injuries to the retroperitoneum [6], peritoneal cavity [2, 4], pelvis and/or spine [5]. Here, we report the case of an isolated LAPA presenting as a delayed hemorrhage in a patient with a single stab wound to the paraspinal region. This lesion was successfully managed with microcoil embolization.
CASE REPORT
An 18-year-old male presented to our institution with a chief complaint of intermittent, recurrent hemorrhage from the right lower paraspinal region, where he had sustained a knife stab 10 days prior. He was initially evaluated at an outside hospital, where he underwent contrast-enhanced computed tomography (CT) scan of his abdomen and pelvis, which demonstrated only soft tissue changes consistent with a superficial stab injury. The wound was sutured, and the patient was discharged from emergency department in hemodynamically stable condition. At his follow-up on Day 9, he had his sutures removed and on the next day noticed blood tracking from the wound down to his ankle. He presented again to the outside institution where no bleeding was visualized, and he was discharged once again. On Day 11, his dressing saturated, and contrast-enhanced CT scan at this time showed active hemorrhage in the soft tissue and musculature lateral to the right paraspinal muscles without involvement of the retroperitoneal space. At that time, the patient was transferred to our institution for further care.
Examination on admission revealed an actively bleeding 2-cm wide stab wound in the right lumbar paraspinal region. A contrast-enhanced CT of the pelvis showed an enhancing lesion consistent with a pseudoaneurysm extending from a branch of a right lumbar artery (Figs 1 and 2). The patient was transferred to the interventional radiology suite where angiography confirmed the diagnosis (Fig. 3). The pseudoaneurysm was then successfully embolized using platinum microcoils (Fig. 4), which were positioned in the lumbar artery, proximal and distal to the origin of the pseudoaneurysm. The patient tolerated the procedure well and was discharged the following day without any further complication.

Contrast-enhanced CT scan of the lower abdomen and pelvis showing a single lobe of a presumed, bilobed pseudoaneurysm (a) as well as a 3.5 × 5.5 × 6 cm rim-enhancing, lobular collection of the superior right gluteal subcutaneous tissues, just superior to the right iliac crest and lateral to the paraspinal musculature, consistent with a hematoma (b).

Axial cut from the same contrast-enhanced CT scan of the lower abdomen and pelvis showing a 1.6-cm bilobed, enhancing lesion, consistent with pseudoaneurysm, presumably extending from a branch of a right lumbar artery (a).
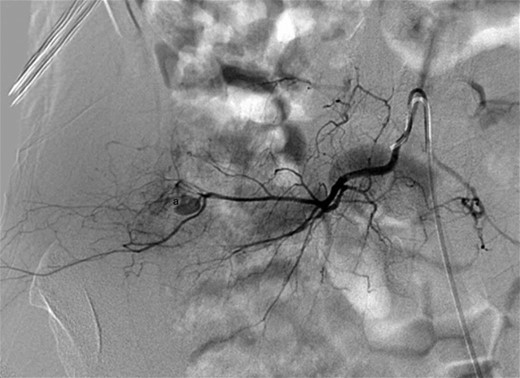
Digital subtraction angiography showing a small pseudoaneurysm originating from the peripheral aspect of the distal right lumbar artery (a).
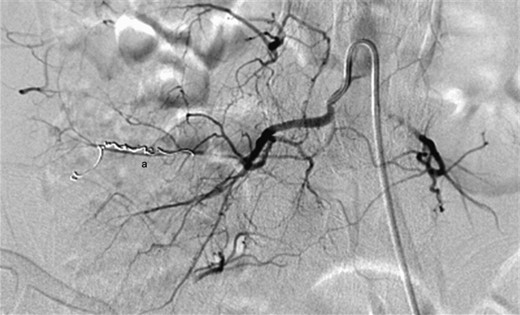
Digital subtraction angiography demonstrating successful embolization of the proximal and distal entry points of the pseudoaneurysm using platinum microcoils (a).
DISCUSSION
Traumatic pseudoaneurysm of a lumbar artery is an uncommon occurrence and is most often noted in the setting of high-energy, blunt force trauma or penetrating trauma with significant concomitant injury to intra-abdominal structures [2, 4]. A review of the literature suggests the time from injury to presentation of a traumatic LAPA is highly variable [6, 7]. They may present acutely with hemodynamic instability in the setting of an expanding retroperitoneal hematoma [6, 7], or they may present 1–2 weeks after the inciting injury [2, 4, 5]. Some reports document presentations delayed for months [3] or even years after the initial injury [8].
In many reports, the diagnosis of LAPA in the setting of trauma was initially missed, often because of concomitant overshadowing intra-abdominal [2–4] and/or spinal injuries [5]. This study represents an example from the opposite end of the spectrum, wherein the diagnosis was missed on the patient's readmission because of the isolated nature and apparent simplicity of the inciting event. Nevertheless, delayed diagnosis of LAPAs can be life threatening, thus illustrating the necessity of a thorough initial trauma evaluation. Management of a LAPA in a stable patient can often be achieved through endovascular embolization [1, 3] as supported by our case. To our knowledge, this is the first report of such a complication occurring after an isolated paraspinal stab wound, without evidence of any additional injury.
This case emphasizes the importance of maintaining an appropriate index of suspicion in a patient with penetrating trauma and recurrent bleeding and/or pain several days to weeks after initial evaluation. Pseudoaneurysm rupture has the potential to be acutely life threatening, and a thorough trauma evaluation with diligent follow-up care is paramount even for patients with a seemingly uncomplicated pattern of injury.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}