





Abstract
We report a rare case of bronchogenic cyst associated with congenital complete absence of the pericardium. A 17-year-old male was admitted to the hospital for surgical resection of a growing cystic lesion located in the middle mediastinum. The patient was asymptomatic and no significant findings were found on physical examination. Resection of the mediastinal cyst was performed by video-assisted thoracoscopic surgery. The complete absence of the pericardium was immediately observed along with a cystic tumor arising from the mediastinum. After the resection of the cyst, no additional procedure to reconstruct the absence of the left pericardium was performed. Pathological diagnosis was a bronchogenic cyst. Congenital absence of the pericardium may be associated with the bronchogenic cyst and complete absence of the pericardium requires no additional surgical reconstruction, if remaining space in the pleural cavity is small enough to avoid cardiac disposition after surgical resection of the cyst.
INTRODUCTION
Congenital absence of the pericardium is a rare anomaly. In most patients, pericardial defects are asymptomatic and found only during surgery or autopsy [1, 2]. Congenital pericardial defects have also been reported to be associated with other congenital anomalies, including bronchogenic cyst [2, 3]. A bronchogenic cyst is an uncommon congenital cystic lesion of the mediastinum and may be detected during routine chest radiograph without obvious symptoms [4]. We present a rare case of bronchogenic cyst associated with congenital complete absence of the pericardium, the latter detected during video-assisted thoracoscopic surgery.
CASE REPORT
A 17-year-old man was admitted to the hospital for surgical resection of an enlarging mediastinal cystic mass. A routine medical examination carried out at a junior high school detected an abnormal shadow on chest radiograph and chest computed tomography (CT) scan showed a cystic lesion (25 × 23 mm) located on the lateral side of the aortic arch in the middle mediastinum with no other abnormalities. Gradual growth of the cystic lesion was discovered by a CT scan during follow-up over 3 years with the lesion reaching 38 × 33 mm in size (Fig. 1). The patient was asymptomatic with no significant findings on physical examination. An electrocardiogram (ECG) on admission showed right bundle branch block (RBBB) with no other abnormal findings, and spirometry showed normal respiratory function.

Preoperative chest CT scan showing a cystic mediastinal mass adjacent to the left pulmonary artery and aortic arch.
Resection of the cystic mass was performed by video-assisted thoracoscopic surgery with a three-port approach on the left side. As left ventricle and left atrial appendage were directly visualized, the complete absence of the pericardium was immediately observed. The cystic mass arising from the middle mediastinum was attached to the pulmonary artery and visceral pleura of the left upper lobe, and dissected using an electric cautery (Fig. 2). No additional procedure was performed to reconstruct the pericardial defect following the resection of the cyst. The postoperative course was uneventful. The chest tube was removed on the third postoperative day and the patient was discharged on the fifth postoperative day. Pathological diagnosis was a bronchogenic cyst and turbid fluid content was contained in the cyst (Fig. 3).
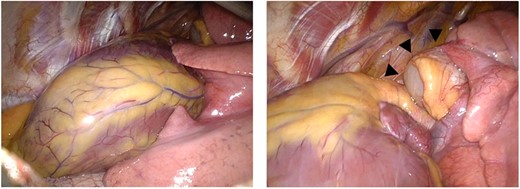
Intraoperative thoracoscopic images. Complete absence of the left pericardium (left) and cystic mass (arrow heads) arising from the middle mediastinum (right).
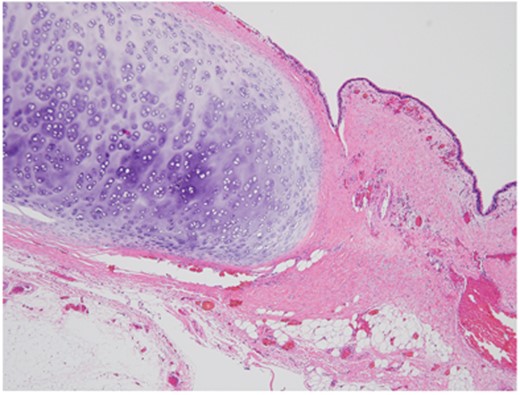
Microscopic view of resected bronchogenic cyst showing ciliated epithelium and cartilage (H&E stain, ×20).
DISCUSSION
Congenital absence of the pericardium is a rare anomaly and in most cases, discovered during surgery. The prevalence has been reported as only 1 in 14 000 autopsies at Johns Hopkins [1] or 15 in 34 000 patients undergoing cardiovascular surgery at Mayo Clinic (0.044%) [2]. The developmental mechanism is unclear, but may be due to failure of pericardial development secondary to premature atrophy of the left duct of the cardinal vein, which then fails to nourish the left pleuropericardial membrane [5].
Congenital pericardial defects may be associated with other congenital anomalies, including patent ductus arteriosus, atrial septal defect, tetralogy of Fallot, mitral valve stenosis, bronchogenic cyst, pulmonary sequestration, pectus excavatum and diaphragmatic hernia [2]. Although congenital absence of the pericardium is rarely diagnosed preoperatively, there have been some reports describing the usefulness of imaging modalities, such as magnetic resonance imaging or echocardiogram [6, 7]. Displacement of the cardiac silhouette to the left on chest radiograph and RBBB on ECG are also common findings in patients with the complete absence of the left pericardium [8]. In our case, the patient was asymptomatic with a RBBB on ECG suggesting the absence of the pericardium. In most cases, complete absence of the pericardium is asymptomatic and the patient is at no risk. However, with a partial absence of the pericardium, there is a possible risk of fatal myocardial strangulation due to herniation of the left ventricle or atrial appendage and surgical intervention such as closure or enlargement of the pericardial defect may be required [7].
Including this case, there have been reports of 18 cases of patients with the bronchogenic cyst associated with congenital pericardial defect [3]. In all patients, pericardial defect was asymptomatic and discovered only during surgery. A bronchogenic cyst is rare congenital cystic lesion in the mediastinum or lung parenchyma and can be asymptomatic [4]. Complete surgical resection is generally preferred due to the risk of enlargement or possible infection. In cases of bronchogenic cyst with the absence of the pericardium, partial absence of the left pericardium was predominant and to our knowledge, there have been three reports (two were reported in English) describing complete absence of the pericardium including this case [3].
In cases with complete pericardial defect, the requirement for pericardial reconstruction is patient-dependent. It has been reported that no additional fixation of the complete pericardial defect was required following surgical resection of a giant pulmonary cyst because appropriate expansion of the lung to stabilize the heart was expected [9]. However, another report describes how severe postoperative cardiac displacement was seen in a patient following a left upper lobectomy [10]. In our patient, the absence of space in the pleural cavity following resection of the bronchogenic cyst indicated that fatal disposition of heart was unlikely to happen. As a result, no additional procedure was carried out to cover the pericardial defect.
In conclusion, congenital pericardial defect may be associated with the bronchogenic cyst and in most cases, it is asymptomatic. In contrast with partial absence of the pericardium, complete absence of the pericardium has a less risk of fatal complications even in the absence of additional surgical reconstruction. However, to avoid fatal cardiac displacement, pericardial reconstruction may be required if surgical resection results in additional space in the pleural cavity allowing extra mobility of the heart.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}