





Abstract
Endometriosis is the presence of endometrial tissue outside the uterine cavity. It has been previously reported in the abdominal wall secondary to gynaecological surgery. We present the case of a 32-year woman with endometrioma of the abdominal wall masquerading as an intramuscular lipoma with no previous surgical history.
INTRODUCTION
Endometriosis was described by Rokitansky and is defined as the presence of functioning endometrial tissue outside the uterine cavity. It occurs in up to 15% of menstruating women and is usually located within the pelvis [1]. Extra-pelvic endometriosis has been reported in the peritoneum, liver, bowel, urinary tract and thorax [2]. Abdominal wall endometriosis is rare and is usually seen following a gynaecological surgical procedure allowing endometrial tissue to be transplanted [3]. Endometriosis of the abdominal wall may be difficult to diagnose and it can be misdiagnosed as a hernia, lipoma or granuloma. We present the interesting case of a patient with an endometrioma of the abdominal wall with no previous surgical history.
CASE REPORT
A 32-year-old lady was referred to our clinic with complaints of a painful lower abdominal lump. It had been present for 4 months and had become more symptomatic over time. She had a past medical history of hyperthyroidism but nothing else of note. Abdominal examination revealed a 2-cm infra-umbilical palpable lump within the left rectus muscle which was mildly tender and did not have a cough impulse. An ultrasound scan showed a hard 2 × 3 cm lesion in her left rectus and no evidence of a hernia (Fig. 1). To characterize the lesion further, an magnetic resonance imaging (MRI) scan was organized and it revealed a benign lesion consistent with an intramuscular lipoma (Fig. 2). She was taken to the theatre for excision of the lump. Intra-operatively she was found to have an inflammatory mass and therefore a wide excision was carried out. The patient was discharged with no complications. Histological examination revealed endometriosis of the abdominal wall. She has been followed for 6 months with no signs of a recurrence.
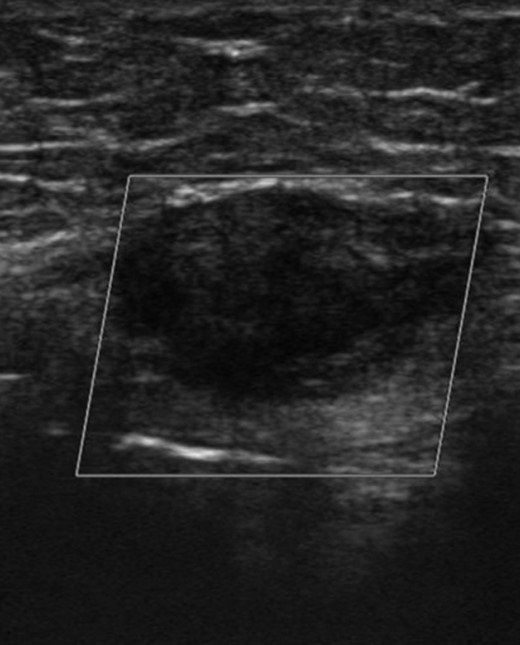
Ultrasound scan showing a hard 2 x 3cm lesion in her left rectus.
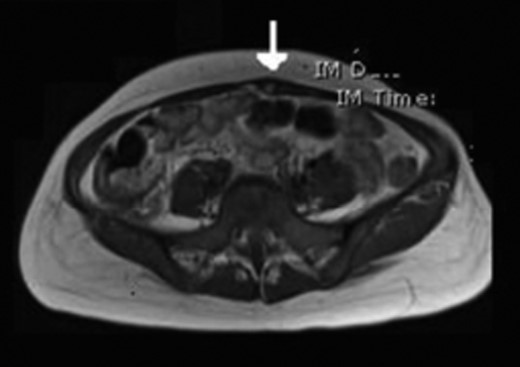
MRI showing a benign lesion consistent with an intramuscular lipoma.
DISCUSSION
Endometriosis was described by Rokitansky and is defined as the presence of functioning endometrial tissue outside the uterine cavity. It occurs in up to 15% of menstruating women and is usually located within the pelvis [1]. Endometriosis of the abdominal wall is a rare occurrence and is usually related to a previous gynaecological surgical procedure. Interestingly our patient did not have any past surgical history and there is only one similar report in the literature [4]. Different pathophysiological theories concerning the origins of endometriosis have been proposed, including the implantation or reflux, direct extension, embryonic rest (claiming a specific stimulus to a Mullerian origin cell nest produces endometriosis) and lymphatic and vascular metastasis [5]. It is a difficult condition to diagnose pre-operatively due to its rarity and non-specific symptoms and signs. Even though some patients complain of cyclical pain, it has also been reported as being a constant focal pain unrelated to menses [6]. This was the case in our patient which made a pre-operative diagnosis extremely difficult.
Pre-operative imaging techniques include ultrasonography (US), computerized tomography (CT) and MRI. US can help in excluding other pathologies such as a hernia, haematoma or abscess [7]. The CT and MRI characteristics of abdominal wall endometrioma are non-specific and therefore those investigations cannot be used as diagnostic tools [8]. Pre-operative biopsy can be carried but the preferred management is wide local excision [9]. Follow-up is recommended as local recurrence can occur and is most likely due to inadequate surgical excision [10].
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}