





Abstract
Most clinicians throughout the world are probably unaware of the existence of masticatory muscle tendon-aponeurosis hyperplasia (MMTAH), potentially leading to misdiagnoses such as temporomandibular joint disorder (TMD). Here, we introduce this disease from the viewpoint of education. In February 2013, a 39-year-old woman presented with limited mouth opening. Her facial configuration was characterized by a square mandible. There was no evidence of TMD. Magnetic resonance imaging (MRI) showed bilateral enlargement of the masseter muscles. Additionally, a ‘thick’ aponeurosis of the anterior aspect of the masseter muscle was noted bilaterally. On maximal mouth opening, intraoral palpation along the anterior border of the masseter muscle confirmed a hard cord-like structure, consistent with the findings on MRI. MMTAH was diagnosed. When clinicians notice limited mouth opening on oral examination, they should be knowledgeable about diseases associated with limited mouth opening and a square mandibular configuration, such as MMTAH.
INTRODUCTION
Limited mouth opening is a common health problem that interferes with eating, speech and oral hygiene [1]. The causes of limited mouth opening include trauma, infection, temporomandibular joint disorders (TMDs), neurological disorders, rheumatoid arthritis, drugs, tumors, hyperplasia of the coronoid process, etc. This condition can interfere with various medical treatments that require access to the oral cavity. Masticatory muscle tendon-aponeurosis hyperplasia (MMTAH), a rare cause of limited mouth opening, is a new disease entity which has been recently established [2–4]. At present, most clinicians are not yet aware of this disease, leading to the risk of misdiagnosis as other diseases, such as masseter muscle hypertrophy and TMDs. Consequently, patients with MMTAH have been treated inappropriately. Here, we present a case of MMTAH.
CASE REPORT
In February 2013, a 39-year-old woman presented with limited mouth opening suspected by her dentist to be caused by TMD. She could not open her mouth widely since her elementary school days, and restricted mouth opening gradually developed. She always ate sushi after tearing it into small pieces. Her facial configuration was characterized by a square mandible (Supplementary Video 1). Oral examination revealed no pain on motion, tenderness, clicking or injury of the temporomandibular joint. The lower jaw moved smoothly, but unaided maximal mouth opening was only 27 mm (Supplementary Video 1). There was thus no evidence of TMDs. Magnetic resonance imaging (MRI) showed bilateral enlargement of the masseter muscles. In addition, a ‘thick’ aponeurosis of the anterior aspect of the masseter muscle was noted bilaterally (Fig. 1). On maximal mouth opening, intraoral palpation along the anterior border of the masseter muscle confirmed a hard cord-like structure, consistent with the findings on MRI. MMTAH, recently established disease category [2–4], was thus diagnosed.
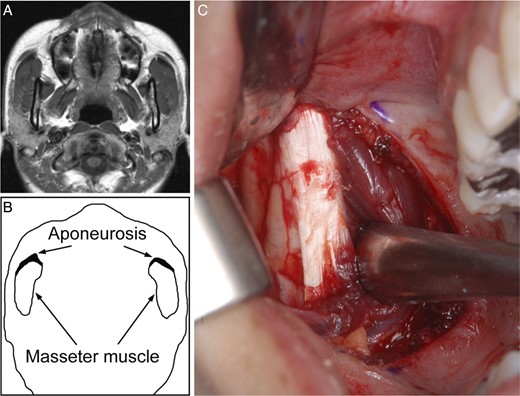
The characteristics of MMTAH. (A) MRI on horizontal section at the middle level of face. (B) Scheme illustrating bilateral ‘thick’ aponeurosis on the anterior of masseter muscle. (C) Right ‘thick’ aponeurosis before resection during surgery.
After obtaining her consent, surgical treatment was performed (Figs 1 and 2; Supplementary Video 2). Resection of the ‘thick’ masseter muscle aponeurosis and coronoidectomy, performed under general anesthesia, increased maximal mouth opening from 29 to 53 mm. Although the coronoid process did not interfere with the zygomatic bone on mouth opening, the coronoidectomy was needed to completely resect the temporal muscle tendon from the posterior of the coronoid process. Five days after surgery, postoperative mouth-opening training began. The current mouth opening is 49 mm (Supplementary Video 3).

Right temporal muscle tendon before resection during surgery.
DISCUSSION
MMTAH was designated as a new disease entity by the Japanese Society for Oral and Maxillofacial Surgeons in 2005. However, most clinicians throughout the world are probably unaware of the existence of MMTAH, potentially leading to misdiagnoses such as TMD. Consequently, patients with MMTAH might receive inappropriate treatment. For example, resection of a portion of the masseter muscle was previously reported not to improve limited mouth opening in a patient with bilateral masseter muscle hypertrophy [5]. Although both MMTAH and masseter muscle hypertrophy present with muscle hypertrophy, these two diseases differ substantially because masseter muscle hypertrophy is not accompanied by limited mouth opening. The aforementioned case is thus suspected to be MMTAH. A diagnosis of typical MMTAH requires bilateral ‘thick’ aponeuroses on the anterior aspect of the masseter muscle as confirmed by intraoral palpation and MRI, as well as slowly progressing limited mouth opening, which often develops in childhood. MMTAH is frequently accompanied by a square mandibular configuration with mandibular angle hypertrophy due to the hyperplastic aponeurosis and tendon. The limited mouth opening associated with MMTAH is due to extension disturbance of the muscles, resulting from hyperplasia of tendons and aponeuroses, which appear normal histopathologically [1]. We have performed the procedure described above followed by mouth-opening training in 34 patients since 2000. Good results were achieved in >95% of patients. According to our investigation, the ratio of MMTAH among about 1000 persons in Japanese elementary and junior high schools was ∼1% (unpublished data).
Anesthesiologists have also reported problems in laryngoscopy during the induction of anesthesia in patients undergoing surgery for MMTAH [6]. Recently, Lehman et al. reported that four female patients who had presented with limited mouth opening and lateral and protrusive movements within normal limits had been treated by bilateral coronoidectomy with the significant improvement of limited mouth opening. We consider that these cases must be MMTAH [7].
When clinicians notice limited mouth opening on oral examination, they should be knowledgeable about diseases associated with limited mouth opening and a square mandibular configuration, such as MMTAH.
SUPPLEMENTARY MATERIAL
Supplementary material is available at Journal of Surgical Case Reports online.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}