





Abstract
Meckel's diverticulum is a remnant of the omphalomesenteric duct and is the most common congenital anomalies of the gastrointestinal tract. It has been known to mimic different disease states making its diagnosis difficult. Common complications consist of bleeding, intestinal obstruction and inflammation. The patient discussed in this case study was a 29-year-old Hispanic female who presented with right lower quadrant abdominal pain. A CT scan showed a normal appendix, thickened terminal ileum and a high-grade distal small bowel obstruction with a possible closed-loop obstruction. Laparoscopy revealed Meckel's diverticulum with the rare complication of torsion. The mechanism of torsion has been postulated but with little evidence. The purpose of this case report is to discuss the apparent mechanism of axial torsion secondary to the presence of a mesodiverticular band, provide visual evidence at surgery and recommend all Meckel's diverticulum associated with a mesodiverticular band be resected to prevent further complications.
INTRODUCTION
Meckel's diverticulum occurs in 1–3% of the population and is the most common congenital anomaly of the gastrointestinal tract [1]. It is a remnant of the omphalomesenteric duct, which connects the primitive gut to the yolk sac in early development and is normally obliterated by the 7th- to 8th week of gestation. Meckel's diverticulum has been known to follow the ‘rule of 2's’. This memory tool indicates that the diverticulum will be ∼2 inches long and 2 feet from the ileocecal valve, occurs in 2% of the population, commonly presents in the first 2 years of life and may have two types of epithelial tissue.
The most common complications of Meckel's diverticulum in children and adults are lower gastrointestinal hemorrhage and diverticulitis, respectively. Other complications include intestinal obstruction, perforations, Littre's hernia and tumors [2]. Axial torsion of the diverticulum is a rare complication that has only been reported seven times in adults previously [3, 4]. Torsion of the diverticulum is associated with both omphalomesenteric and mesodiverticular bands. While the omphalomesenteric band is a remnant of the omphalomesenteric duct, the mesodiverticular band is an embryologic remnant of the vitelline circulation. Persistence of this embryological structure, which arises from the superior mesenteric artery, leads to an arterial band that can be patent. The band extends from adjacent mesentery to the apex of the diverticulum [5]. This creates an opening through which bowel loops may herniate and become obstructed. The purpose of this case report is to discuss the apparent mechanism of axial torsion around a mesodiverticular band, as well as a proposal of protocol for management.
CASE REPORT
A 29-year-old female presented with a 5-day history of right lower quadrant abdominal pain. The pain was constant, dull and did not radiate. On physical examination, the patient appeared to be anxious and uncomfortable. There was moderate right lower quadrant tenderness, rebound tenderness and guarding. Complete blood count revealed leukocytosis with a predominance of neutrophils. A CT scan was performed and showed a normal appendix with a thickened terminal ileum. There also appeared to be a distal small bowel obstruction with a possible closed-loop obstruction.
Laparoscopy was performed and a large Meckel's diverticulum was identified ∼30 cm proximal from the ileocecal valve. It had twisted 360° and was swollen and gangrenous at the distal half (Fig. 1). The tip of the diverticulum contained a 3-cm long mesodiverticular band that was attached to the mesentery of an adjacent loop of terminal ileum (Fig. 2). The mesodiverticular band was surgically divided, and the diverticulum was then de-torsed revealing a normal appearing base (Fig. 3). The diverticulum was excised along its base using an endoscopic stapler (Fig. 4). The surgery was completed with an appendectomy. On postoperative day one, the patient was doing well and was discharged home.

Axial rotation and gangrene of the Meckel's diverticulum.

Mesodiverticular band connecting the tip of the Meckel's diverticulum to adjacent small bowel mesentery.

De-torsed diverticula revealing a normal appearing base.

Excised Meckel's diverticulum before removal from the abdomen.
DISCUSSION
Meckel's diverticulum is the most common congenital anomaly found in the gastrointestinal tract. Its presence may result in complications such as bleeding, bowel obstruction and inflammation. Axial torsion is a rare complication that has only been reported in seven cases prior to this study. In the case presented here, the findings at laparoscopy support a specific mechanism for the development of torsion. The patient was found to have an internal hernia under a bridge formed by the mesodiverticular band. Based on these findings, it is believed that the connection between the mesodiverticular band and adjacent mesentery establishes an axis for diverticular torsion and an opening for bowel to herniate, thus propagating the important mechanism for pathology (Fig. 5). Herniation often leads to obstruction and could be detrimental if left untreated as the bowel wall becomes edematous, perfusion is decreased and absorptive function is lost.
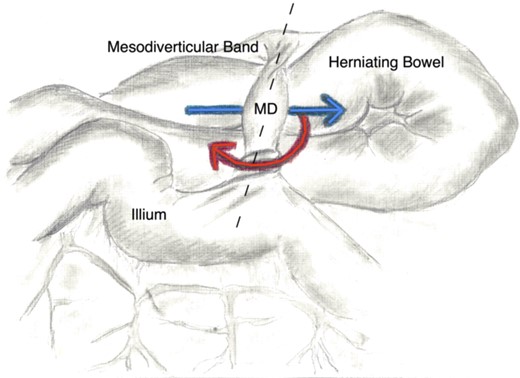
This illustration depicts the mechanism of torsion and small bowel herniation. The red line represents the rotation of the Meckel's diverticulum (MD) around axis created by the mesodiverticular bands attachment to adjacent mesentery and the ilium (the dotted line). The blue arrow shows the path in which the bowel herniates and thus propagating the rotation of the MD.
Current recommendations regarding management of Meckel's diverticulum are controversial, but include resection in all symptomatic patients and asymptomatic children when found during the course of an abdominal exploration. It is recommended not to electively resect the diverticulum when found incidentally on imaging in children or adults, as well as, in asymptomatic patients >50 years of age when found during the course of an abdominal exploration [6]. Some physicians advocate the use of a numerical scoring system to assess risk for complication and need for intervention [7]. Regardless of the method used to assess proper intervention, we believe that all Meckel's diverticulum that present with concomitant mesodiverticular bands should be resected to prevent future morbidities associated with this congenital anomaly.
CONFLICT OF INTEREST STATEMENT
None declared.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}